Meniscus Surgery NYC — Repair & Meniscectomy Specialists
Written by: Dr. Popovitz.
Board-Certified Orthopedic Surgeon | Fellowship-Trained Sports Medicine, NYU Langone Medical Center | FAAOS
Co-Founder, NY Bone & Joint Specialists | Lenox Hill Hospital - Northwell Health
Recognized: New York Magazine Best Doctor | New York Times Super Doctor | IAOS Leading Physician of the World | IAOS Top Orthopedic Surgeon in New York
Date Published: May 4, 2026
Last Updated: May 4, 2026
Last Medically Reviewed: May 4, 2026
This page has been written and reviewed by a fellowship-trained, board-certified orthopedic surgeon with over 20 years of clinical experience. All clinical claims are supported by peer-reviewed literature and current AAOS and AOSSM guidelines. See References section below.
At a glance
Meniscus surgery is a minimally invasive arthroscopic procedure used to repair or remove damaged cartilage in the knee, helping restore stability and function. It treats both traumatic and degenerative meniscus tears, including those occurring with ACL injuries. At New York Bone & Joint, Dr. Leon Popovitz and a fellowship-trained surgical team perform these procedures at Lenox Hill Hospital, with care coordinated across Upper East Side and Midtown offices. Recovery depends on the procedure, ranging from a few weeks to several months, with progress based on functional milestones. New York Bone & Joint reports a 95% meniscus repair healing rate, exceeding typical benchmarks, reflecting a preservation-focused approach and integrated rehabilitation.
Book a consultation
Prompt Appointments Available
Upper East Side: 1198 Third Ave | Midtown: 425 Madison Ave
Surgery performed at Lenox Hill Hospital - Northwell Health
About this page
This page was written and is maintained by Leon Popovitz, MD, a board-certified orthopedic surgeon and co-founder of New York Bone & Joint Specialists, fellowship-trained in sports medicine at NYU Langone Medical Center. Dr. Popovitz specializes in knee surgery and sports medicine with more than 20 years of clinical practice in New York City. New York Bone & Joint is a private orthopedic surgery and sports medicine practice with two Manhattan locations — Upper East Side (1198 Third Avenue) and Midtown (425 Madison Avenue). Meniscus surgery is performed at Lenox Hill Hospital, part of the Northwell Health system. New York Bone & Joint is independent of hospital systems and operates as a physician-founded private practice.
A torn meniscus is one of the most common knee injuries we treat—and one of the most important decisions you will make is whether to repair it or remove part of it.
At New York Bone & Joint Specialists, meniscus preservation is not a tagline. It’s the clinical foundation of everything we do. Led by Dr. Leon Popovitz our team of fellowship-trained orthopedic surgeons has spent over 20 years building a practice around one conviction: that preserving your meniscus safely is the single most important factor in the long-term health of your knee joint. Remove the meniscus unnecessarily, and it will accelerate the path to arthritis. Repair it, and you will protect the joint.
Dr. Popovitz is a board-certified orthopedic surgeon who was also fellowship-trained in sports medicine at NYU Langone Medical Center, is a Fellow of the American Academy of Orthopaedic Surgeons (FAAOS), and is a former team physician for the US Open Tennis Championships. Over 20 years in practice, he has personally performed meniscus surgery for professional athletes, competitive sport athletes, and active adults of all ages, repairing acute traumatic tears in young athletes to degenerative tears in patients hoping to avoid knee replacement.
Every physician at New York Bone & Joint operates with the same preservation-first philosophy. Our 5-year surgical outcome data reflects this: a 95% meniscus repair healing rate (compared to the published benchmark of 70–90%) built on precise tissue assessment, meticulous technique, and a rehabilitation protocol coordinated directly between your surgeon and our in-house physical therapy team.
Already evaluated and told you need meniscus surgery? You do not need to start over. New York Bone & Joint offers prompt surgical consultations and second opinions so you can move forward confidently, or get the clarity you need before committing to a procedure. If you have a new knee injury and are not yet sure what you are dealing with, our sports medicine physicians can evaluate you quickly (even same day or next day) and then connect you with a surgeon promptly if indicated.
Introduction
A torn meniscus is among the most common orthopedic injuries we see at New York Bone & Joint Specialists, and it’s among the most misunderstood. Many patients are told they need surgery immediately. Others are told to wait indefinitely. What is almost never communicated clearly is the most important fact in meniscus management: whether you repair the meniscus or remove part of it is a decision with decades-long consequences for your knee. [1]
At New York Bone & Joint, our fellowship-trained knee surgeons have performed meniscus surgery for over 20 years, treating traumatic tears in young athletes, degenerative tears in active adults, and complex root tears that other practices have mismanaged or missed. Our surgical philosophy is built on a single principle: repair whenever possible, remove only what is absolutely necessary. Based on our own 5-year surgical outcome data, our meniscus repair healing rate is 95% (compared to the published benchmark of 70–90%). That gap is not accidental. It reflects an intraoperative tissue assessment that goes beyond what MRI can show, and a rehabilitation protocol coordinated between your surgeon and our in-house physical therapy team from day one.
New York Bone & Joint surgeons perform meniscus surgery at Lenox Hill Hospital, one of Manhattan’s premier surgical facilities, while consultations, imaging, and physical therapy take place at our Upper East Side and Midtown offices. If you have already been evaluated and recommended for meniscus surgery, you do not need to start over. We offer prompt surgical consultations and second opinions. If you have a new knee injury and are not yet sure what you are dealing with, one of our sports medicine physicians can evaluate you quickly and give you a clear picture of your options the same day.
What Is the Meniscus and Why Does It Matter?
The meniscus is not a minor structure. Each knee has two: a medial meniscus on the inner side and a lateral meniscus on the outer side. Together, they perform functions that no artificial implant can fully replicate. They cushion the impact between the femur and tibia, distribute load across the knee joint, stabilize the knee during rotation, and protect the articular cartilage that lines the joint surface. [1]
When the meniscus is removed in whole or part, those functions are lost. The articular cartilage is exposed to forces it was never designed to bear alone. Over time, this leads to progressive cartilage loss and, ultimately, osteoarthritis. The research is very clear on this point. [5] [7] This is why the decision between repair and removal is not a technical preference but rather a decision that shapes the long-term health of your knee.
Types of Meniscus Tears
Not all meniscus tears are the same, and the type of tear determines both the treatment approach and the urgency with which it must be addressed.
| Tear Type | Description | Typical Cause | Treatment Direction |
| Radial | Tears across the width of the meniscus, disrupting its hoop stress function. Even small radial tears can compromise the meniscus’s load-bearing ability. | Acute twisting injury; common in younger athletes | Repair strongly preferred. Radial tears at the body can compromise the entire meniscus if not repaired. |
| Bucket-Handle | A large, longitudinal tear where a section of meniscus flips into the joint, causing locking and loss of full extension. Surgical urgency. | Acute injury, often with ACL tear | Surgical repair. The displaced fragment must be reduced and repaired. |
| Posterior Root Tear | A tear at the bony attachment point of the meniscus. Functionally equivalent to removing the entire meniscus and leads to rapid arthritis progression if unrepaired. [4] | Sudden deep squat or deceleration; degenerative in older patients | Repair is essential. Root repair prevents the 4.64x increased risk of accelerated osteoarthritis associated with unrepaired root tears. [4] |
| Horizontal / Flap | Tears that split the meniscus horizontally, creating an unstable flap. Common in degenerative tears in middle-aged patients. | Degenerative, cumulative wear | Repair if tissue quality allows. Partial meniscectomy if not. |
| Degenerative | Fraying or partial tears without a clear single injury event. Often seen on MRI in patients with knee pain, but may be incidental. | Age-related wear, often associated with early arthritis | Non-operative management first. Surgery is only recommended if mechanical symptoms persist after physical therapy. |
“An important clinical nuance that MRI alone cannot always resolve: the same tear can look very different in the operating room than it does on imaging. A tear that appears repairable on MRI may prove to have poor tissue quality intraoperatively, meaning it’s frayed, delaminated, or avascular. That can make repair inadvisable. Conversely, a tear that looks borderline on MRI may prove to be in excellent tissue, well within the vascular zone, and highly repairable once we can directly assess it. This is why the repair vs. meniscectomy decision is ultimately an intraoperative one, made by a surgeon experienced enough to assess the tissue in real time.” — Leon Popovitz, MD
Repair vs. Partial Meniscectomy: Why the Decision Matters
The long-term data on partial meniscectomy is sobering. While it reliably relieves mechanical symptoms in the short term, studies consistently show that removal of meniscus tissue, even partial removal, accelerates articular cartilage loss and increases the risk of knee osteoarthritis over a 10–20-year horizon. [7] For younger, active patients in particular, a partial meniscectomy performed today may bring forward the timeline of knee replacement by a decade or more.
Meniscus repair, by contrast, preserves the tissue and its function. Healing rates in the published literature are approximately 70–90% for well-vascularized tears in appropriate candidates. [3] At New York Bone & Joint, based on our own 5-year surgical outcome data, our meniscus repair healing rate is 95%. This reflects our preservation-first approach, precise intraoperative tissue assessment, and directly coordinated post-operative rehabilitation protocol.
The trade-off is recovery time. Meniscus repair requires a more protected recovery than meniscectomy, typically four to six weeks of restricted weight-bearing to allow the repair to heal, with a structured rehabilitation program of a total four to six months before return to sport. For many patients, that additional recovery time is a worthwhile investment in decades of joint health. Our surgeons will walk you through that calculation specifically for your tear, your age, your activity level, and your goals.
Are You a Candidate for Meniscus Surgery?
Not every meniscus tear requires surgery, and not every meniscus tear that requires surgery requires repair. At New York Bone & Joint, we will never recommend an operation unless it is genuinely the right answer for your specific situation.
Meniscus surgery is typically recommended when:
- You have a confirmed traumatic meniscus tear on MRI especially with mechanical symptoms such as locking, catching, giving way, or persistent pain that have not resolved with rest and initial management.
- You have a posterior root tear which we approach with urgency, as unrepaired root tears are associated with a 4.64x increased risk of accelerated knee osteoarthritis. [4] In these cases, we do not recommend waiting.
- You have a bucket-handle tear causing joint locking or a significant loss of knee extension. This is an urgent issue and should be addressed promptly.
- You have a degenerative meniscus tear with persistent mechanical symptoms such as locking, catching, or giving way that have not resolved after an appropriate course of physical therapy and/or injection treatment. [1]
- You have a meniscus tear alongside an ACL injury that requires reconstruction. We address both in the same surgical session.
Meniscus surgery is generally not recommended for patients with a non-traumatic meniscus finding on MRI and no mechanical symptoms, patients with mild degenerative tears and no instability, or patients who have not yet completed a meaningful course of conservative treatment. Some degenerative tears are incidental findings on MRI that are not the actual source of pain. Our surgeons will review your imaging, your symptoms, and your examination findings together and give you a straight answer.
All the while, your New York Bone & Joint surgeons’ core focus will always be on preserving your own tissue. The meniscus is the primary protector of your articular cartilage and your articular cartilage is what stands between you and arthritis. [5]
| From Dr. Popovitz: What an Unrepaired Root Tear Really Means A 39-year-old woman came to see me after seven months of knee pain that had been managed by other providers as ‘early arthritis.’ She had been given a cortisone injection with no relief and then ultimately underwent a knee arthroscopy and a partial meniscectomy. She is a recreational runner and pickleball player. Now, she could not play or even run at all. Her MRI had been read as showing a ‘degenerative’ medial meniscus tear. When I reviewed her MRI myself, I saw a posterior root tear, which is a tear at the exact point where the medial meniscus anchors to the tibial bone. Think of this as like how the roots of a tree anchors it into the ground. The radiology report had noted ‘degenerative changes’ without flagging the root involvement. This is a common and consequential miss, because a root tear is functionally equivalent to removing the entire meniscus. I obtained new x-rays in the office and they already showed some subtle development of arthritis compared to her original X-rays. I repeated the MRI to see how much meniscus was removed during her previous surgery. The new MRI clearly showed the meniscus root tear. The amount of tissue removed by the previous surgeon was not extensive and there was still a considerable amount of meniscus remaining that needed to be saved. If the meniscus root tear would not be repaired then the function of the remaining meniscus would be lost and arthritis would advance rapidly. Again, there was already the beginnings of early progression of arthritis. Therefore, I performed an arthroscopic posterior root repair, reattaching the meniscus back to its tibial footprint. Eight months later, she returned to full activity, including routinely playing in tournaments. Her mild arthritis has not gotten worse on follow-up imaging. I was pleased to see we were able to stop her arthritis from progressing and persevere her tissue. What I think about when I see that case is how different the outcome would have been if the root tear had gone unrepaired for another year or two. The arthritic changes that were just beginning would have accelerated dramatically. A woman in her late thirties would have been on a path to a possible knee replacement in her fifties or sooner. The right diagnosis, made at the right time can change a patient’s life. The focus on preserving tissue is the absolute key to the longevity. — Leon Popovitz, MD |
The Procedure: What Happens During Meniscus Surgery
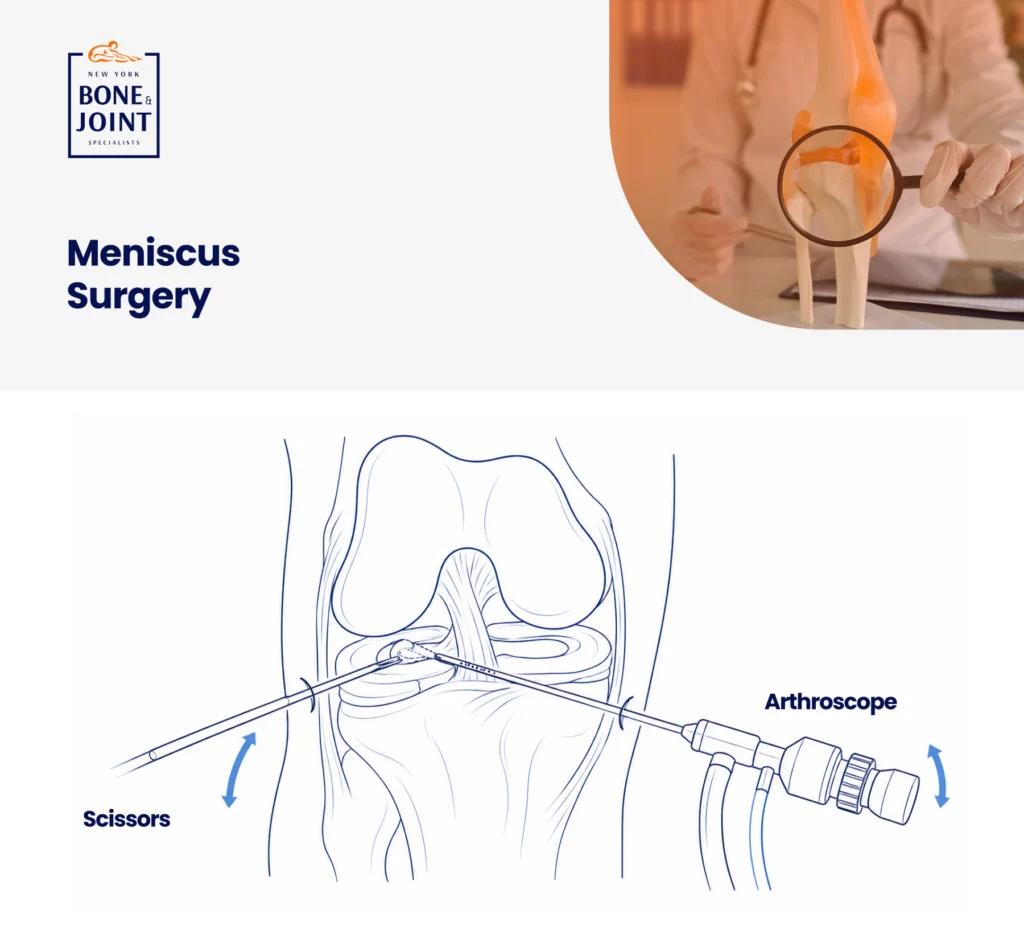
Meniscus surgery with New York Bone & Joint is performed arthroscopically, which is a minimally invasive approach using two or three small portals, a camera, and specialized instruments. Patients go home the same day. Most procedures take between 30 and 60 minutes depending on the tear type, repair complexity, and whether concurrent injuries are addressed. [2]
Your surgeon will:
- Make two or three small portals around the knee, typically less than a centimeter each, to access the joint.
- Perform a complete arthroscopic survey of the entire joint: both menisci, the articular cartilage surfaces, the ACL, PCL, and joint lining. We do not operate on the meniscus in isolation. Concurrent findings are identified and addressed.
- For repair: The torn tissue is prepared and reattached using sutures passed through the tear and anchored to the surrounding tissue or bone. The technique varies by tear type (e.g. inside-out, outside-in, or all-inside repair), which is determined intraoperatively based on tear location and configuration.
- For partial meniscectomy: Only the unstable, irreparable portion of the meniscus is removed using a shaver. Healthy, stable tissue is preserved in all cases. We never remove more than is necessary.
- Address any concurrent cartilage damage, loose bodies, or other findings identified during the joint survey.
- Close the portals with small absorbable sutures and apply a surgical dressing.
“A nuance that matters intraoperatively: the decision to repair versus remove is sometimes finalized in the operating room, not before it. MRI is our best pre-operative tool, but the actual tissue quality, such as vascularity, tensile strength, and tear configuration, is assessed by feel and direct visualization. If the tear is not near the “red zone,” which is where blood flows, then the repair would not heal. Blood flow, in addition to secure fixation, is critical for healing.
“We go into every meniscus case prepared to repair. If the tissue cannot support a durable repair or of the tear is in an area where there is no blood flow to allow healing then we remove only what is necessary. We explain this clearly and in detail before the procedure.” — Leon Popovitz, MD
Recovery & Rehabilitation: What to Expect

Recovery after meniscus surgery depends entirely on whether repair or partial meniscectomy was performed. These are not interchangeable timelines. Your surgeon will provide a procedure-specific protocol at your pre-operative appointment.
| Timeframe | Partial Meniscectomy | Meniscus Repair |
| Days 1–7 | Weight-bearing as tolerated immediately. Ice and elevation for swelling. Most patients walk without crutches within a few days. | Non-weight-bearing or toe-touch weight-bearing. Crutches required. Ice and elevation. Brace if indicated. |
| Weeks 1–2 | Return to desk work typical by day 3–5. PT begins early for range-of-motion and quad activation. | PT begins for gentle range-of-motion and quad sets. No weight-bearing progression yet. |
| Weeks 3–6 | Progressive strengthening and return to low-impact activity. Stationary bike by week 3–4. | Progressive weight-bearing begins. Brace is removed by week 4–6 depending on repair type. Strengthening is begun. |
| Months 2–3 | Most patients return to sport and high-demand activity. Criteria-based clearance: strength and functional testing. | Progressive strengthening. Stationary bike. No pivoting or cutting yet. |
| Months 4–6 | Fully recovered for the majority of patients. | Return to jogging typically by month 4. Sport-specific training begins. Criteria-based clearance for return to sport. |
| Months 6+ | N/A. Most patients are fully recovered before this point. | Full return to sport for most patients. Criteria-based clearance required: strength symmetry testing, functional hop tests, physician sign-off. |
Patients who undergo partial meniscectomy typically return to desk work within three to five days and to low-impact sport within six to eight weeks. Meniscus repair requires a substantially longer, more protected recovery, but for the right tear in the right patient, that investment in recovery time is an investment in decades of joint health.
In-House Physical Therapy: Why It Matters More After Meniscus Repair
After meniscus repair in particular, the rehabilitation protocol is not just important: it’s one of the primary determinants of whether the repair heals. Progress too fast and you risk re-tear. Progress too slowly and you develop stiffness and muscle atrophy that compromises the final outcome. The margin for error is narrower than for most orthopedic procedures.
At New York Bone & Joint, your physical therapist and your surgeon are in the same center and communicate directly about your case from day one. Before your first PT appointment, your therapist has already reviewed your operative report, confirmed the repair type and technique, and spoken with your surgeon about the protection protocol specific to your tear. Your program is built around what was done in the operating room, not a generic ‘post-meniscus repair’ template.
When questions arise during your recovery about weight-bearing, pain, or a sensation that doesn’t feel right, your physical therapist can speak directly with your surgeon the same day, right in the same center. This is the structural advantage of coordinated in-house care, and it matters most in the procedures where precise protocol adherence determines the outcome.
Why Choose New York Bone & Joint for Meniscus Surgery?
| New York Bone & Joint Advantage | What It Means for You |
| 95% meniscus repair healing rate (5-year data) | Based on our own 5-year surgical outcome data, significantly above the published benchmark of 70–90%. This is the result of precise intraoperative tissue assessment, preservation-first decision-making, and coordinated post-operative rehabilitation. |
| Preservation-first philosophy | We go into every meniscus case prepared to repair. We never default to meniscectomy because it is faster or easier. If tissue cannot support a durable repair, we explain why and remove only what is necessary. |
| Intraoperative repairability assessment | We always evaluate repairability in the operating room, not just from MRI. A tear that looks borderline on imaging may prove highly repairable once we can assess the tissue directly. A tear that looks repairable may prove otherwise. This real-time judgment is the difference between experienced meniscus surgery and routine arthroscopy. |
| Root tear expertise | Posterior root tears are the most consequential and most commonly missed meniscus injury. We look for root involvement on every knee MRI we review and treat it with the urgency it warrants. |
| In-house PT at the same center | Your surgeon and physical therapist communicate directly. Repair-specific protocols are built from the operative report, not from a generic template. |
| Prompt consultations | Patients with acute tears are seen promptly. Imaging is coordinated immediately. If a bucket-handle tear needs urgent attention, we act accordingly. |
| Same surgeon, from start to finish | The physician who evaluates you is the surgeon who operates on you and sees you through recovery. No handoffs, no unknown providers. |
| The bottom lineWhen surgery is the right answer for your meniscus, who does it and how they approach the repair vs. removal decision is what determines whether your knee is healthy at 50 or you are facing replacement at 55. New York Bone & Joint’s preservation-first approach, intraoperative tissue assessment, and 5-year outcome data are not marketing claims. They are the clinical record of 20 years of doing this work the right way. |
Risks and Considerations
Meniscus surgery is one of the most commonly performed and safest procedures in orthopedic surgery. As with any surgical procedure, there are risks that should be understood before proceeding.
- Infection: Rare with arthroscopic procedures (less than 1% [9]). Strict sterile technique and post-operative care instructions minimize this risk.
- Re-tear or incomplete healing: Meniscus repair does not succeed in every case. Published healing rates are approximately 70–90% for well-vascularized tears. At New York Bone & Joint, based on our own 5-year surgical outcome data, our healing rate is 95%. Tears in the avascular white zone have lower healing potential and may require partial meniscectomy rather than repair. Your surgeon will explain the expected healing likelihood for your specific tear before the procedure. [3]
- Stiffness: Particularly after meniscus repair with a protected weight-bearing protocol. Early supervised PT with a protocol specific to your repair type significantly reduces this risk.
- Blood clots (DVT): Uncommon after knee arthroscopy, particularly in younger patients. Your surgeon will advise on activity and anticoagulation if relevant to your profile. But anticoagulation is not typically necessary.
At your consultation, your surgeon will walk through the specific risks relevant to your tear type, your anatomy, and your individual health profile.
References
- American Academy of Orthopaedic Surgeons. Meniscus Tears. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/meniscus-tears
- American Academy of Orthopaedic Surgeons. Knee Arthroscopy. OrthoInfo. orthoinfo.aaos.org/en/treatment/knee-arthroscopy
- American Orthopaedic Society for Sports Medicine (AOSSM). Meniscus repair outcomes. aossm.org
- Foreman SC et al. Meniscal Root Tears and Extrusion Are Significantly Associated with the Development of Accelerated Knee Osteoarthritis. Am J Sports Med. 2020. pubmed.ncbi.nlm.nih.gov/32567341
- Lohmander LS et al. The long-term consequence of anterior cruciate ligament and meniscus injuries. Am J Sports Med. 2007. pubmed.ncbi.nlm.nih.gov/17761605
- Pujol N et al. Long-term outcomes of all-inside meniscal repair. Am J Sports Med. 2012. pubmed.ncbi.nlm.nih.gov/23740324
- Lee DH et al. Clinical and radiographic results of partial versus total meniscectomy in patients with symptomatic discoid lateral meniscus: A systematic review and meta-analysis. Orthop Traumatol Surg Res. 2019. pubmed.ncbi.nlm.nih.gov/31027980
- American Academy of Orthopaedic Surgeons. Articular Cartilage Restoration. OrthoInfo. orthoinfo.aaos.org/en/treatment/articular-cartilage-restoration
- Salzler MJ et al. Complications after arthroscopic knee surgery. Am J Sports Med. 2014. pubmed.ncbi.nlm.nih.gov/24284049
FAQs
Not every torn meniscus requires surgery, but some tears, particularly posterior root tears and bucket-handle tears, should be addressed promptly to prevent irreversible joint damage. Degenerative meniscus tears without mechanical symptoms often respond well to physical therapy and activity modification. Traumatic tears especially with locking, catching, or giving way typically do not resolve without surgery. And root tears should not wait. The consequences of leaving a root tear unrepaired is accelerated advancement of arthritis. [4] At your consultation, we will review your MRI and your symptoms and give you a direct answer.
Meniscus repair stitches the torn tissue back together. A meniscectomy removes the torn portion. Repair preserves the meniscus and its function (cushioning, load distribution, joint stabilization and protecting the articular cartilage) which lines the ends of the bones inside the joint. Meniscectomy relieves symptoms faster but removes tissue permanently.
The long-term data consistently shows that meniscectomy accelerates articular cartilage loss and increases arthritis risk over a 10–20-year period. [7] When repair is possible, we repair. When it is not (because the tissue is avascular, degenerated, or structurally unsalvageable) we remove only what is necessary so to preserve as much cartilage as possible.
A posterior root tear is a tear at the bony attachment point of the meniscus, and it is functionally equivalent to removing the entire meniscus. The meniscus extrudes, loses its hoop stress function, and the knee begins progressing toward arthritis immediately. Research shows that unrepaired root tears are associated with the meniscus essentially losing all its function, as though you have lost the entire meniscus. There is a 4.64x increased risk of accelerated knee osteoarthritis. [4] Root tears are frequently misread on MRI as ‘degenerative changes’ by those who may not be particularly experienced in this type of tear and are not specifically looking for root involvement. At New York Bone & Joint, we review every knee MRI for root pathology and treat it with the urgency it warrants.
Recovery after partial meniscectomy is rapid. Most patients return to desk work within three to five days and to sport within six to eight weeks. Meniscus repair recovery is longer and more protected: restricted weight-bearing for four to six weeks, progressive strengthening through months two through four, and return to sport with criteria-based clearance at four to six months. The repair timeline is longer by design: the repair needs protected time to heal, and the investment in recovery is an investment in decades of joint health.
Yes. When a meniscus tear is present alongside an ACL tear, we address both in the same surgical session. Meniscus tears occur alongside ACL tears in 40–70% of cases. A repaired meniscus actually has a higher healing rate when repaired simultaneously with ACL reconstruction, because the bone tunnel drilling releases stem cell-rich marrow that supports tissue healing. We always assess the meniscus on pre-operative MRI and inspect it directly during ACL reconstruction.
Based on New York Bone & Joint’s own five-year surgical outcome data, our meniscus repair healing rate is 95%, compared to the published benchmark of 70–90% for well-vascularized tears in appropriate candidates. [3] Success depends significantly on tear location (vascular red zone vs. avascular white zone), tissue quality, patient age, and adherence to the post-operative rehabilitation protocol. Your surgeon will discuss the expected healing likelihood for your specific tear before the procedure.
Some meniscus tears, such as small, stable tears in the outer vascular zone, can heal without surgery if given adequate rest and time. However, the majority of symptomatic tears, particularly those with mechanical symptoms, do not heal on their own. Degenerative tears in the avascular inner zone will not heal regardless of rest, but many can be managed non-operatively if they are not causing mechanical symptoms. Root tears and bucket-handle tears do not heal without surgical repair and should not be left unaddressed. [1]
Yes. MRI is the standard imaging required to assess tear type, location, tissue quality, and surgical planning before meniscus surgery. In cases involving suspected root tears, we may also request weight-bearing X-rays to assess for early joint space narrowing and meniscal extrusion. New York Bone & Joint is affiliated with MRI facilities across the New York area and can coordinate a prompt appointment in a location convenient to you. We review every MRI ourselves. We do not rely solely on radiology reports for meniscus cases.
Medically Reviewed by Dr. Popovitz.
You can book your appointment with New York Bone & Joint online by submitting the appointment request form here:
Book an appointmentOur Locations
-

Upper East Side: Full Service Orthopedic Center & Walk-In
1198 3rd Avenue, Between 69th and 70th Street New York, NY 10021Physician appointments: Mon–Fri 9am–5:30pm, Sat 8:30am–4:30pm
Physical therapy: Mon–Fri 7am–7pm, Sat 8am–2pmPhone: (212) 759-4553 -

Orthopedic Doctor Midtown Manhattan NYC — New York Bone & Joint Specialists
425 Madison Ave, Suite 200 (second floor) New York, NY 10017 (corner of East 49th Street)Physician appointments: Mon–Fri 8:00 am–6:00 pm
Physical therapy: Mon–Fri 7 am–7 pm, Sat 8 am–2 pmPhone: (212) 759-4553 -

Orthopedic Doctor Upper East Side NYC — New York Bone & Joint Specialists
130 E 67th St New York, NY 10065Physician appointments: Mon–Fri 8:00am–6pm, Sat 8:30am–4:30pm
Physical therapy: Mon–Fri 7am–7pm, Sat 8am–2pmPhone: (212) 759-4553