Gel Injections NYC — Hyaluronic Acid & Viscosupplementation at New York Bone & Joint
Written by: Dr. Popovitz.
Board-Certified Orthopedic Surgeon | Fellowship-Trained Sports Medicine, NYU Langone Medical Center | FAAOS
Co-Founder, NY Bone & Joint Specialists | Lenox Hill Hospital - Northwell Health
Recognized: New York Magazine Best Doctor | New York Times Super Doctor | IAOS Leading Physician of the World | IAOS Top Orthopedic Surgeon in New York
Date Published: May 5, 2026
Last Updated: June 4, 2026
Last Medically Reviewed: June 4, 2026
This page has been written and reviewed by a fellowship-trained, board-certified orthopedic surgeon with over 20 years of clinical experience. All clinical claims are supported by peer-reviewed literature and current AAOS and AOSSM guidelines. See References section below.
At a glance
- What it is: An injection of hyaluronic acid, a substance that occurs naturally in healthy joint fluid, directly into a joint to supplement the lubrication lost in osteoarthritis, reduce pain, and improve joint function. Also called viscosupplementation or a gel shot.
- FDA approval: Gel injections are FDA-approved for knee osteoarthritis only. Use in other joints such as hip, shoulder, and ankle is off-label, physician-directed, and supported by published evidence but not FDA-cleared. [9]
- Who is it for at New York Bone & Joint: Patients with knee osteoarthritis who have not responded adequately to cortisone, have reached appropriate frequency limits for cortisone, or want to avoid repeated cortisone injections. Also: younger patients with patellofemoral syndrome who have failed physical therapy and are not appropriate candidates for cortisone. [5]
- Who performs it: New York Bone & Joint sports medicine physicians for most indications; orthopedic surgeons when the injection is part of a surgical evaluation or broader treatment plan. All procedures at both Manhattan offices, no hospital visit required.
- What to expect: Relief typically begins 4–8 weeks after completing the injection series, with studies showing sustained pain reduction for 6–12 months or longer for knee OA. [3] Duration varies by individual, disease severity, and activity level.
- Important: Gel injections treat symptoms of joint degeneration but don’t reverse cartilage loss or repair structural damage. They are a non-surgical tool to manage pain and maintain function, not a cure.
- Insurance: Most major insurance plans cover gel injections for knee OA when medically indicated. Coverage for off-label use varies. Coverage verified before your procedure.
Book a consultation
Prompt Appointments Available
Upper East Side: 1198 Third Ave | Midtown: 425 Madison Ave
Surgery performed at Lenox Hill Hospital - Northwell Health
About this page
This page was written and is maintained by Leon Popovitz, MD, co-founder of New York Bone & Joint Specialists, a board-certified orthopedic surgeon fellowship-trained in sports medicine at NYU Langone Medical Center. Gel injections and viscosupplementation at New York Bone & Joint are administered by our sports medicine physicians and orthopedic surgeons. New York Bone & Joint is a private orthopedic surgery and sports medicine practice with two Manhattan locations — Upper East Side (1198 Third Avenue) and Midtown (425 Madison Avenue). New York Bone & Joint is physician-founded and independent of hospital systems.
Introduction
Gel injections (hyaluronic acid, or viscosupplementation) are one of the most effective and most misunderstood non-surgical options in orthopedic medicine. They aren’t a first-line treatment for joint pain. They aren’t a substitute for physical therapy. And they aren’t cortisone. They’re a specific tool, used for specific patients, at a specific point in the non-surgical treatment pathway. [1]
At New York Bone & Joint Specialists, we use gel injections in three primary situations: for patients with knee osteoarthritis who haven’t responded adequately to cortisone or who have reached the appropriate frequency limits for corticosteroid injections; for patients who want to avoid the documented cartilage risks associated with repeated cortisone in a weight-bearing joint; and for younger patients with patellofemoral syndrome who have failed physical therapy and are not appropriate candidates for cortisone because of their age. In all three situations, the gel injection is used because it’s the right tool for that patient, not because it’s the easiest or the default.
The goal, as it is across every non-surgical procedure at New York Bone & Joint, is to exhaust every appropriate option before surgical intervention is considered. For the right patient, a well-timed gel injection series can provide 6–12 months of meaningful pain relief, allow continued activity, and delay or avoid the need for surgery. That is a clinically significant outcome, provided the patient is correctly selected and honestly counseled about what to expect.
What is a Gel Injection and How Does it Work?
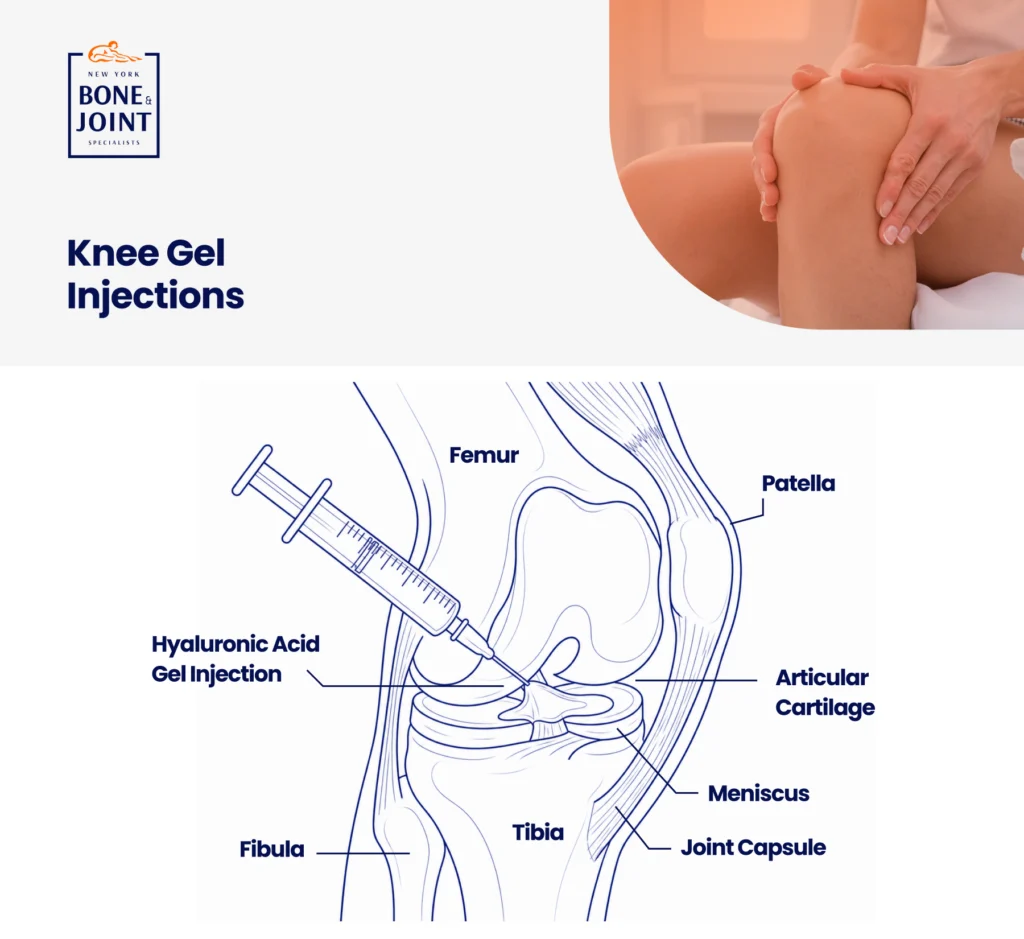
Hyaluronic acid is a naturally occurring substance found throughout the body, with the highest concentration in the synovial fluid that lubricates joints. In a healthy joint, hyaluronic acid acts as both a lubricant and a shock absorber, allowing the joint surfaces to move against each other smoothly and absorb impact. In osteoarthritis, the concentration and quality of hyaluronic acid in the joint fluid degrades, meaning the fluid becomes thinner and less viscous, the joint loses its natural lubrication, and the mechanical and inflammatory damage of arthritis accelerates.
A gel injection replenishes this degraded hyaluronic acid by delivering a viscous, gel-like solution directly into the joint space. This isn’t purely mechanical. Beyond restoring lubrication, hyaluronic acid injections are thought to have anti-inflammatory properties, may stimulate the joint’s own hyaluronic acid production, and may have a direct protective effect on articular cartilage. [4] The result, for the right patient, is a reduction in pain and improvement in joint function that can outlast the physical presence of the injected material in the joint, which is why relief from a gel injection often lasts significantly longer than relief from cortisone.
“The important distinction between gel and cortisone is timing and mechanism. Cortisone works quickly, reducing inflammation directly. Most patients feel relief within 3–5 days. Gel works slower. The full benefit often takes 4–6 weeks to manifest, but the relief tends to last longer and doesn’t carry the cartilage risk associated with repeated corticosteroid injections. [7] [10] I think of them as different tools for different stages of the same problem. When a patient asks me which one they should have, my answer is always: it depends on where you are in the disease course and what your treatment history looks like.” — Leon Popovitz, MD
When Gel Injections are the Right Choice Instead of Cortisone
This is the clinical decision that most patients and many providers get wrong. Cortisone and hyaluronic acid are not interchangeable. Each has specific appropriate indications, and choosing the right one requires understanding where the patient is in their disease course.
| Consider gel injections instead of (or after) cortisone in these situations Cortisone has stopped working or the relief duration is shortening: When a patient has received multiple cortisone injections and each one provides less relief than the last, continuing cortisone is not the answer. The diminishing response signals that the inflammatory component is no longer the dominant driver of the pain and that the joint itself needs a different type of support. Gel injections are the appropriate next step. [1] Appropriate frequency limits for cortisone have been reached: Repeated intra-articular corticosteroid injections in weight-bearing joints are associated with accelerated cartilage loss and osteoarthritis progression. [7] When a patient has reached the point where additional cortisone carries more risk than benefit, gel injections provide a non-corticosteroid alternative for continued non-surgical pain management. The patient is too young for the cartilage risks of repeated cortisone: For younger patients with knee OA or patellofemoral syndrome, the long-term consequences of repeated corticosteroid injections (documented cartilage volume loss over 2 years [10]) are more consequential than they are for an older patient. In these patients, gel injections provide meaningful symptom relief without the documented risks of cortisone at high frequency. Patellofemoral syndrome that has failed PT: Younger patients with patellofemoral syndrome who have completed an appropriate course of physical therapy without adequate improvement are often not candidates for cortisone injections because of their age and the specific anatomy of the patellofemoral joint. Hyaluronic acid injection has published evidence for symptom relief in this population. [5] This is one of the most important and most underutilized indications for gel injections. Patient preference to avoid cortisone: Some patients have medical reasons to avoid corticosteroids (poorly controlled diabetes, prior adverse reactions) or simply prefer to avoid repeated steroid exposure. Gel injections are a legitimate alternative when the indication is appropriate. |
“I find gel injections most valuable for the patients who have already been through cortisone. The cortisone helped initially, then started helping less, and they have been asking themselves what comes next that isn’t surgery. That is exactly the patient gel injections were designed for. The other group I think about a lot is the younger patient with patellofemoral pain. These are active people in their 20s and 30s who cannot run or go up and down stairs without pain, who have done everything their physical therapist has asked, and who are not surgical candidates. Cortisone in the patellofemoral joint in a 28-year-old isn’t something I’m comfortable with. But a gel injection series? That is an evidence-based option I can offer with confidence.” — Leon Popovitz, MD
Conditions Treated With Gel Injections at New York Bone & Joint
| Condition | Joint | FDA Status | What to Expect |
| Knee Osteoarthritis (mild to moderate) | Knee | FDA-approved | Best evidence base for gel injections. Studies show 28–54% pain reduction vs. baseline. [4] Most effective for mild to moderate OA; less effective for bone-on-bone end-stage arthritis. Relief typically 6–12 months. [3] |
| Patellofemoral Syndrome (failed physical therapy, younger patients) | Patellofemoral joint (knee) | FDA-approved (knee) | Published evidence supports symptomatic relief when physical therapy has been exhausted. [5] New York Bone & Joint uses this as a specific indication for younger patients who are not appropriate candidates for cortisone. Relief duration variable. |
| Hip Osteoarthritis | Hip | Off-label | Published evidence supports pain relief for hip OA. [8] Requires image guidance (ultrasound or fluoroscopy) for accurate placement. Off-label use discussed with patient before proceeding. |
| Shoulder Osteoarthritis / Glenohumeral OA | Shoulder | Off-label | Some evidence for shoulder OA symptom relief. Off-label. Used at physician discretion when other conservative measures have failed. |
| Ankle Osteoarthritis | Ankle | Off-label | Limited but supportive evidence for ankle OA. Off-label. Ultrasound guidance used. |
| FDA approval status. What it means for you: Gel injections are FDA-approved as a medical device (not a drug) for knee osteoarthritis only. [9] The FDA approval is specifically for pain associated with OA of the knee in patients who have not had adequate response to conservative treatment and simple analgesics. Use in the hip, shoulder, or ankle is off-label, meaning it is not FDA-cleared for those joints but it is legal, widely practiced, and supported by published clinical evidence. Before any off-label injection, your New York Bone & Joint physician will discuss the evidence, the approval status, and the risks and benefits with you directly. |
Gel Injection Products: Single Injection vs. Series
Several FDA-approved hyaluronic acid products are available for knee osteoarthritis, differing primarily in the number of injections in a treatment course and the molecular weight of the hyaluronic acid. Studies comparing single-injection products to multi-injection series have shown comparable clinical outcomes for most patients. [6] Your physician will recommend the product and course that best fits your clinical situation, imaging findings, and treatment history.
| Product Type | Injection Schedule | Examples | Clinical Notes |
| Single-injection | One injection per treatment cycle | Monovisc, Synvisc-One, Gel-One | Convenience advantage. Comparable efficacy to multi-injection series for most patients. [6] |
| 3-injection series | One injection per week for 3 weeks | Euflexxa, Supartz, Hyalgan | More established evidence base. Gradual buildup may suit patients who want a staged approach. |
| 5-injection series | One injection per week for 5 weeks | Synvisc, Orthovisc | Longest established history. Some evidence of superior duration in certain patient populations. |
Treatment cycles can typically be repeated after 6 months if the first cycle provided meaningful relief. The decision to repeat is based on the duration and degree of relief from the prior cycle, the current state of the joint on examination and imaging, and whether the patient’s overall clinical picture has changed.
| From Dr. Popovitz: Two Patients, Two Different Reasons for the Same Injection The golfer: A 58-year-old retired accountant who plays golf three or four times a week came to see me after two years of managing his right knee pain with cortisone injections at another practice. The first injection had been excellent: four months of good relief. The second, about six months later, gave him three months. The third gave him about six weeks. He was worried he was heading for knee replacement. When I examined him and reviewed his imaging, he had moderate medial compartment osteoarthritis. Significant, but not bone on bone. He wasn’t a surgical candidate at this point, and I didn’t think he needed to be. The diminishing cortisone response was a signal, not a dead end. It told me the acute inflammatory component was no longer the dominant driver of his pain: the degenerative joint changes were. That’s exactly the situation gel injections were designed for. We completed a course of hyaluronic acid injections. At eight weeks, he was back to his full golf schedule with significantly reduced pain. He has now completed three treatment cycles over two years, each providing approximately six to eight months of meaningful relief. He hasn’t needed surgery. The runner: A 34-year-old woman came to see me with anterior knee pain that had been present for seven months. She was a regular runner who had been unable to run at all. Going up and down stairs was painful enough to affect her daily life. She had completed four months of physical therapy with a good physical therapist, done everything correctly, and had not improved enough to return to running. Her MRI showed patellofemoral chondromalacia (that is, cartilage softening on the underside of the kneecap) consistent with patellofemoral syndrome. She was 34 years old. Cortisone in the patellofemoral joint of a 34-year-old is not a treatment I’m comfortable offering routinely. The documented cartilage risk from repeated corticosteroid injections matters more at 34 than it does at 64. But she had failed physical therapy and needed something.We administered a hyaluronic acid injection series into the patellofemoral joint. At six weeks she was running again: four miles at a time. She completed a half marathon four months later. These two patients are the ones I think about when someone asks me who gel injections are for. Not every patient with knee pain. The patient who has been through cortisone and needs what comes next. And the patient who is too young for cortisone and needs something between physical therapy and surgery. — Leon Popovitz, MD |
What to Expect: Before, During, and After
Before the Injection
Your New York Bone & Joint physician will review your symptoms, examine the affected joint, and confirm that gel injection is the appropriate next step based on your diagnosis, imaging, and treatment history. Recent X-ray or MRI is typically reviewed before proceeding. You don’t need to fast or prepare specially. Take your regular medications unless specifically instructed otherwise.
During the Injection
Each injection takes approximately 10–15 minutes. The skin is cleaned and a local anesthetic may be applied to the entry site. Ultrasound guidance is used where it improves accuracy of placement, particularly for hip, ankle, and deep knee injections. The hyaluronic acid is injected directly into the joint space. The procedure is generally well tolerated. Most patients describe mild pressure rather than significant pain. You are awake throughout and go home immediately after. [1]
After the Injection
You may experience mild swelling or discomfort at the injection site for 24–48 hours. Avoid strenuous activity for 48 hours post-injection. Unlike cortisone, gel injections do not typically provide immediate relief. The full benefit builds over 4–8 weeks. Most patients begin to notice improvement in the second to fourth week after completing the series.
Risks and Considerations
Hyaluronic acid injections are generally well tolerated with a low risk of serious adverse events. [1] Specific risks to understand:
- Post-injection flare: A temporary increase in joint pain and swelling for 24–48 hours after injection, caused by a local reaction to the injected material. More common with certain products. Resolves without intervention in the vast majority of cases. Ice and rest help.
- Pseudoseptic reaction: A rare but more significant inflammatory reaction producing warmth, swelling, and pain in the joint. Must be distinguished from joint infection. If a joint becomes hot, very swollen, and painful after a gel injection, contact New York Bone & Joint promptly. Most of the time the reaction resolves with a course of non-steroidal anti-inflammatory medication such as Motrin or Aleve.
- Infection: Very rare with standard sterile technique. Less than 1 in 10,000 procedures.
- Incomplete or no response: Not every patient responds to gel injections. Patients with severe, end-stage osteoarthritis (bone-on-bone) typically do not respond well as there is insufficient joint space for the material to provide meaningful lubrication. If gel injections do not provide relief after an appropriate trial, that result guides the next conversation about options.
- Not appropriate for joint infection or inflammatory arthritis flare: Gel injections shouldn’t be administered into a joint that is actively infected or in the midst of a severe inflammatory arthritis flare. Your physician will screen for these contraindications before proceeding.
Why Choose New York Bone & Joint for Gel Injections?
| New York Bone & Joint Advantage | What it Means for You |
| Right patient, right treatment, right time | We don’t offer gel injections as a default response to joint pain. We offer them when the clinical picture specifically supports them: failed or frequency-limited cortisone, cartilage concern in a younger patient, patellofemoral syndrome after failed physical therapy. The indication matters. |
| Patellofemoral syndrome expertise | New York Bone & Joint specifically uses gel injections for younger patients with PFS who have failed physical therapy and are not candidates for cortisone. This is an underutilized indication that we apply with clinical precision. [5] |
| Ultrasound guidance where it matters | Hip, ankle, and complex knee injections are performed with ultrasound guidance at New York Bone & Joint to confirm accurate placement. |
| Honest expectations | We tell you when gel injections are likely to help, when they’re unlikely to help (end-stage OA), and what the difference in onset and duration looks like compared to cortisone. |
| Integrated with orthopedic surgeons | If your gel injection series runs its course and surgical evaluation becomes appropriate, the orthopedic team is in the same center. No new referral, no starting over. |
| Cortisone-to-gel transition expertise | For patients who have been on cortisone and need the next step, our team manages the transition with a clear plan and realistic expectations for each option. |
| No hospital visit | All injections performed in-office at Upper East Side and Midtown offices. |
References
- American Academy of Orthopaedic Surgeons. Viscosupplementation Treatment for Arthritis. OrthoInfo. orthoinfo.aaos.org/en/treatment/viscosupplementation-treatment-for-knee-arthritis
- American Academy of Orthopaedic Surgeons. Arthritis of the Knee. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/arthritis-of-the-knee
- Bannuru RR et al. Therapeutic trajectory following intra-articular hyaluronic acid injection in knee osteoarthritis. Am J Sports Med. 2011. pubmed.ncbi.nlm.nih.gov/21443958
- Altman RD et al. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: a systematic review. BMC Musculoskeletal Disorders. 2015. pubmed.ncbi.nlm.nih.gov/26503103
- Anil U et al. The efficacy of intra-articular injections in the treatment of knee osteoarthritis: A network meta-analysis of randomized controlled trials. Knee. 2021. pubmed.ncbi.nlm.nih.gov/34500430
- Dıraçoğlu D et al. Single versus multiple dose hyaluronic acid: Comparison of the results. J Back Musculoskelet Rehabil. 2016. pubmed.ncbi.nlm.nih.gov/27257981
- Kompel AJ et al. Intra-articular corticosteroid injections in the hip and knee: perhaps not as safe as we thought? Radiology. 2019. pubmed.ncbi.nlm.nih.gov/31617798
- Wu B et al. Efficacy of intra-articular hyaluronic acid injections in hip osteoarthritis: a meta-analysis of randomized controlled trials. Oncotarget. 2017. pmc.ncbi.nlm.nih.gov/articles/PMC5689731
- U.S. Food and Drug Administration. 510(k) clearances for hyaluronic acid knee products. fda.gov
- McAlindon TE et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain. JAMA. 2017. pubmed.ncbi.nlm.nih.gov/28510679
FAQs
A gel injection for the knee is an injection of hyaluronic acid (a naturally occurring joint lubricant) directly into the knee joint to reduce pain and improve function in osteoarthritis, a procedure called viscosupplementation. [1] Hyaluronic acid supplements the degraded synovial fluid in an arthritic knee, restoring lubrication and providing anti-inflammatory effects. [4] Gel injections are FDA-approved for knee osteoarthritis and are used at New York Bone & Joint when cortisone is no longer appropriate, frequency limits have been reached, or the patient is too young for repeated corticosteroid injections.
Cortisone is an anti-inflammatory steroid that reduces joint inflammation quickly: most patients feel relief within 3–5 days; gel injections are hyaluronic acid that supplements joint lubrication and works more slowly, with full benefit taking 4–8 weeks, but typically lasting significantly longer. [7] Cortisone has documented cartilage risk with repeated use in weight-bearing joints. [7] [10] Gel injections do not carry this risk, making them the preferred option for younger patients and those who have reached the appropriate frequency limits for cortisone. The two are not interchangeable; they are different tools for different stages of the same condition.
Most patients with knee osteoarthritis experience meaningful pain relief for 6–12 months after a gel injection series, with some patients reporting benefit beyond 12 months. [3] Duration varies by disease severity, the specific product used, the patient’s activity level, and individual response. Patients who respond well can typically repeat the treatment cycle after 6 months. Those who experience very short-lived relief of less than 3 months may not be ideal candidates for repeat injection.
Gel injections are FDA-approved as a medical device for knee osteoarthritis only, not for other joints including the hip, shoulder, or ankle. [9] Use in non-knee joints is off-label, meaning it is not FDA-cleared but is legal, widely performed, and supported by published clinical evidence. [8] At New York Bone & Joint, the FDA approval status of any injection is discussed with the patient before proceeding, and off-label injections are offered only when the clinical evidence supports them and the patient is fully informed.
Yes, hyaluronic acid injections have published evidence for symptomatic relief in patellofemoral syndrome when physical therapy has been exhausted, and New York Bone & Joint specifically uses them for younger patients with PFS who are not appropriate candidates for cortisone. [5] Patellofemoral syndrome in a younger, active patient is one of our most important indications for gel injections. Cortisone carries documented cartilage risk with repeated use, and a 28-year-old runner is not a patient we want on a long-term cortisone schedule. Gel injections provide a meaningful, lower-risk alternative.
Gel injections are generally not effective for severe, end-stage osteoarthritis with minimal remaining joint space because there is insufficient room in the joint for the hyaluronic acid to provide meaningful lubrication. [1] The best candidates are patients with mild to moderate OA who still have measurable joint space on X-ray. For end-stage OA, the conversation shifts to surgical options, and the orthopedic team at New York Bone & Joint is in the same center to have that conversation when it becomes appropriate. Nevertheless, some patients choose to try the gel injections as one of their last options before proceeding with surgery and in our experience have had some relief.
Depending on the product, a gel injection course is either a single injection or a series of 3 to 5 weekly injections, with single-injection products showing comparable efficacy to multi-injection series for most patients. [6] After completing the initial course, most patients who respond well can repeat the treatment after 6 months. Your New York Bone & Joint physician will recommend the specific product and schedule based on your joint, your clinical picture, and your treatment history.
Generally, gel and cortisone injections are not administered simultaneously into the same joint; the two are typically used sequentially, with cortisone as the earlier intervention and gel as the next step when cortisone is no longer the right choice. Your physician may in some cases recommend a cortisone injection first to reduce acute inflammation before starting a gel series, but this is a case-by-case clinical decision.
Most major insurance plans cover hyaluronic acid injections for knee osteoarthritis when medically indicated, with documented OA on imaging and documented failure of conservative treatment. Coverage for off-label use in non-knee joints is less consistent and varies by insurer. NYBJ will verify your specific coverage before scheduling and provide a clear picture of any out-of-pocket responsibility in advance.
Medically Reviewed by Dr. Popovitz.
You can book your appointment with New York Bone & Joint online by submitting the appointment request form here:
Book an appointmentOur Locations
-

Upper East Side: Full Service Orthopedic Center & Walk-In
1198 3rd Avenue, Between 69th and 70th Street New York, NY 10021Physician appointments: Mon–Fri 9am–5:30pm, Sat 8:30am–4:30pm
Physical therapy: Mon–Fri 7am–7pm, Sat 8am–2pmPhone: (212) 759-4553 -

Orthopedic Doctor Midtown Manhattan NYC — New York Bone & Joint Specialists
425 Madison Ave, Suite 200 (second floor) New York, NY 10017 (corner of East 49th Street)Physician appointments: Mon–Fri 8:00 am–6:00 pm
Physical therapy: Mon–Fri 7 am–7 pm, Sat 8 am–2 pmPhone: (212) 759-4553 -

Orthopedic Doctor Upper East Side NYC — New York Bone & Joint Specialists
130 E 67th St New York, NY 10065Physician appointments: Mon–Fri 8:00am–6pm, Sat 8:30am–4:30pm
Physical therapy: Mon–Fri 7am–7pm, Sat 8am–2pmPhone: (212) 759-4553