A torn rotator cuff is one of the most disabling shoulder injuries you can face, and one of the most consequential decisions you will make is who repairs it and how.
At New York Bone & Joint Specialists, rotator cuff repair is one of the core surgical procedures our practice was built around. Led by Dr. Leon Popovitz, our fellowship-trained surgical team has performed arthroscopic rotator cuff repair for over 20 years for professional athletes, overhead sport athletes, active adults, and manual workers who depend on their shoulder for their livelihood. Our conviction, from the first consultation to the last physical therapy session, is the same as it is across every procedure we perform: that preserving your own tissue is the key to the longevity of your shoulder and your overall health. We repair whenever we can. We maximize every square millimeter of tendon coverage. And when we operate, we operate to produce an outcome that lasts.
Dr. Popovitz is a board-certified orthopedic surgeon fellowship-trained in sports medicine at NYU Langone Medical Center and a Fellow of the American Academy of Orthopaedic Surgeons (FAAOS). Rotator cuff repair is one of his primary subspecialties. With more than 20 years in practice, he has performed all-arthroscopic repairs across the full spectrum of tear sizes, from small partial-thickness tears to large and massive full-thickness tears requiring tendon mobilization and specialized repair constructs. He has served as former team physician for the US Open Tennis Championships and has treated shoulder injuries at the professional, collegiate, and recreational levels. He has been recognized by New York Magazine as a Best Doctor, by the New York Times as a Super Doctor, and by the International Association of Orthopedic Surgeons as both a Leading Physician of the World and Top Orthopedic Surgeon in New York.
Our outcomes reflect this commitment. Based on our own surgical outcome data, New York Bone & Joint’s rotator cuff re-tear rate is 2–4% (compared to published benchmarks of 10–20%), and 94% of our patients report high satisfaction with significant improvements in pain, strength, and range of motion following surgery.
Already evaluated and recommended for rotator cuff repair? You don’t need to start over. New York Bone & Joint offers prompt surgical consultations and second opinions. If you have an acute shoulder injury and aren’t sure what you’re dealing with, our sports medicine physicians can evaluate you same day or next day if needed and connect you with a surgeon promptly if indicated.
Introduction
A torn rotator cuff is one of the most common reasons patients come to see us at New York Bone & Joint Specialists, and one of the most important surgical decisions in orthopedics to get right. The rotator cuff is the foundation of shoulder function. When it tears, the consequences ripple outward: pain, weakness, loss of overhead ability, and progressive joint degeneration that can make later repair impossible if left untreated. [1]
At New York Bone & Joint, our fellowship-trained shoulder surgeons have performed arthroscopic rotator cuff repair for over 20 years, treating tears across the full spectrum: from small partial-thickness tears in young overhead athletes to massive tears in patients in their 60s and 70s who were told elsewhere that their tendon was irreparable. Our all-arthroscopic approach combines precise footprint reconstruction, double-row suture anchor technique where indicated, and a rehabilitation protocol coordinated directly with our in-house physical therapy team. Based on our own surgical outcome data, our rotator cuff re-tear rate is 2–4% (compared to published benchmarks of 10–20%), and 94% of our patients report high satisfaction with significant improvements in pain, strength, and range of motion following surgery.
New York Bone & Joint surgeons perform rotator cuff repair at Lenox Hill Hospital, one of Manhattan’s premier surgical facilities. Consultations, imaging, and physical therapy take place at our Upper East Side and Midtown offices. If you have already been evaluated and recommended for rotator cuff repair, you don’t need to start over. We offer prompt surgical consultations and second opinions. If you have a new shoulder injury, our sports medicine physicians can evaluate you quickly and connect you with a surgeon promptly if indicated.
What Is the Rotator Cuff and Why Does It Matter?
The rotator cuff is a group of four muscles and their tendons (the supraspinatus, infraspinatus, teres minor, and subscapularis) that originate on the shoulder blade and attach to the head of the humerus. Together they form a continuous sleeve of tendon tissue around the humeral head, stabilizing the ball in the socket and powering the rotation and elevation that make the shoulder the most mobile joint in the body. [1]
When any part of this sleeve tears, the mechanical balance of the shoulder is disrupted. The degree of disruption depends on which tendon tears, how much of it, and how long it goes without repair. A small supraspinatus tear in a 40-year-old overhead athlete has a very different prognosis than a massive three-tendon tear in a 65-year-old whose shoulder has been weakening for years. Understanding that distinction is the first thing a rotator cuff specialist brings to your care, and it determines whether repair is the right answer, what technique achieves the best outcome, and what you can realistically expect from recovery.
Types of Rotator Cuff Tears
The type, size, and chronicity of your tear are the three most important factors in surgical planning. Not all tears are treated the same way.
| Tear Type | Description | Common Cause | Surgical Approach |
| Partial-Thickness, Bursal Side | Tear involves the top (bursal) surface of the tendon. Often caused by impingement from a bone spur above. | Repetitive overhead activity; bone spur; age-related degeneration | Debridement if <50% thickness; repair if ≥50% or symptomatic after conservative treatment. [7] |
| Partial-Thickness, Articular Side | Tear involves the bottom (articular) surface of the tendon. More common in overhead athletes and younger patients. | Overhead athletics; internal impingement; repetitive eccentric loading | In situ repair or takedown and full repair depending on thickness and tissue quality. [7] |
| Full-Thickness, Small / Medium (<3cm) | Complete tear through the full thickness of the tendon. Tendon retraction is typically minimal. Best healing potential. | Acute injury; years of progressive degeneration | Single-row or double-row arthroscopic repair. Excellent outcomes in this group. [4] |
| Full-Thickness, Large (3–5cm) | Large tear often involving more than one tendon. More retraction, more tendon mobilization required intraoperatively. | Degenerative; often missed for years before presentation | Double-row repair with tendon mobilization. Footprint coverage is the primary technical priority. [8] |
| Massive (≥5cm or ≥3 tendons) | Tear involving three or more tendons, often with significant retraction, muscle atrophy, and fatty infiltration. The most technically demanding repair in shoulder surgery. | Chronic degeneration; acute-on-chronic injury; prior failed repair | Arthroscopic repair using tendon mobilization, margin convergence, and augmentation where needed. Candidacy assessed individually. [6] |
| Irreparable Tear | Tendon tissue is too retracted, atrophied, or degenerated to be reattached to bone. Requires a different approach. | Severe chronic degeneration; prior failed repair; massive fatty infiltration | Tendon transfer, superior capsular reconstruction, or biological augmentation discussed at consultation. |
“A clinical nuance that MRI alone cannot always resolve: the size and retraction seen on MRI frequently underestimates the intraoperative complexity of large and massive tears. A tear that appears repairable on imaging may prove, once the joint is open, to have more retraction, more fatty infiltration, or poorer tissue quality than anticipated. Conversely, a tear that looks borderline on MRI may prove achievement of full footprint coverage with the right mobilization technique. The repair decision is finalized in the operating room, by a surgeon with the experience and the technical repertoire to adapt in real time. Whatever the circumstance, the key is to preserve the tissue that you have. Otherwise, aside from weakness and pain, the joint can degenerate.” — Leon Popovitz, MD
Why Rotator Cuff Repair and Why Timing Matters
Rotator cuff tears do not heal on their own. Without repair, most tears progress over time and become larger, retract further, and accumulate the fatty infiltration and muscle atrophy that make later repair progressively more difficult and ultimately impossible. [1] This is the fundamental reason we take rotator cuff tears seriously even in patients who are managing their pain: the window for a successful repair closes, and when it closes, the options narrow considerably.
For full-thickness tears in active patients, the published data shows that early repair before significant retraction and fatty infiltration (which develops progressively if the torn tendon is not repaired [15]) is associated with significantly better healing rates and functional outcomes than delayed repair. [5] The tissue is more pliable, the mobilization is less extensive, and the footprint coverage achieved is more complete. We discuss timing as a specific clinical factor in every surgical consultation, not just as a general recommendation.
| Why the re-tear rate matters more than most patients realize A repaired rotator cuff that re-tears has not healed. The patient still has a torn rotator cuff and now faces the prospect of revision surgery on tissue that is more scarred, more retracted, and more technically challenging than the original repair. Published re-tear rates after rotator cuff repair range from 10–20% overall, rising significantly for larger tears and older patients. [4] Based on our own surgical outcome data, New York Bone & Joint’s rotator cuff re-tear rate is 2–4% ( for non-massive tears). That’s the result of precise footprint reconstruction, optimal suture anchor placement, attention to tissue mobilization, and a post-operative rehabilitation protocol that protects the repair during the critical early healing period. When fatty infiltration develops in the cuff musculature, it does not improve after repair, which makes early intervention the most effective protection against long-term functional loss. [16] |
Are You a Candidate for Rotator Cuff Repair?
Not every rotator cuff tear requires surgery. At New York Bone & Joint, we will not recommend repair unless it’s genuinely the right answer for your specific situation.
Rotator cuff repair is typically recommended when:
- You have a confirmed full-thickness tear on MRI with persistent pain and functional limitation that has not responded to physical therapy and/or corticosteroid injection. [1]
- You have an acute, traumatic full-thickness tear, especially in an active patient under 60, where early repair is associated with significantly better healing outcomes. [5]
- You have a large or massive tear where delay risks further retraction, fatty infiltration, and progression to an irreparable state. We discuss the urgency of timing explicitly for these cases.
- You have a partial-thickness tear of 50% or greater thickness, or a symptomatic partial tear that hasn’t responded to conservative treatment. [7]
- You are an overhead athlete or a patient whose livelihood depends on full shoulder function, and non-operative management has not restored that function.
Rotator cuff repair isn’t generally recommended for patients with asymptomatic tears found incidentally on MRI, patients with minimal functional limitation from small partial tears, or patients with significant glenohumeral arthritis where joint preservation is no longer realistic. We will discuss all of these factors at your consultation and give you a straight answer about whether surgery is the right next step.
Our core focus, as always, is preservation. We operate when surgery gives your shoulder the best long-term outcome. We don’t operate when it does not.
| From Dr. Popovitz: Three Patients, One Conviction I think about rotator cuff surgery differently depending on who is sitting across from me. The 32-year-old baseball pitcher with a partial articular-sided supraspinatus tear, the one who hasn’t been able to pitch without pain for eight months, is a completely different conversation from the 61-year-old retired teacher with a large full-thickness tear she has been living and suffering with in an effort to avoid surgery. And both are different from the 57-year-old contractor who came to me after 11 months of pain, who had been given multiple cortisone injections, and went through months of physical therapy with no improvement. By that point, he couldn’t lift his arm above shoulder height or do the overhead work his business depended on. The contractor is the case that stays with me from that period. When I reviewed his MRI myself, I saw a full thickness tear with the beginnings of retraction and early fatty infiltration beginning in the supraspinatus. The window wasn’t closed, but it was closing. Another six months of cortisone and we would have been having a very different conversation about what was still possible. We performed an arthroscopic repair, extensive tendon mobilization with double-row suture anchor construct to maximize footprint coverage. He was protected for four weeks in a sling and in a structured post-operative physical therapy program for six months. At nine months post-surgery he was back on job sites doing full overhead work. What I want every patient to understand is that a rotator cuff tear doesn’t wait. The tissue doesn’t stay the same while you decide. The tendon retracts like a torn rubber band. It often atrophies, which shrinks the available healthy tissue for repair. Moreover, fat infiltrates the retracted tendon and, once established, that fatty infiltration is irreversible. [15] [16] That also diminishes the amount of healthy tissue available for repair. The accumulation of these factors, while surgery is delayed, makes the repair harder and healing less reliable. The right time to repair a torn rotator cuff is when the biology still supports a good outcome, and that window isn’t open indefinitely. That’s the conversation I have with every patient. Not “you need surgery.” But “here is your tear, here is what it will look like in six more months, and here is what is still possible today.” That’s the conversation that lets people make the right decision for their own life. My goal will always be to preserve your own tissue so you can have it for a long lifetime to come. — Leon Popovitz, MD |
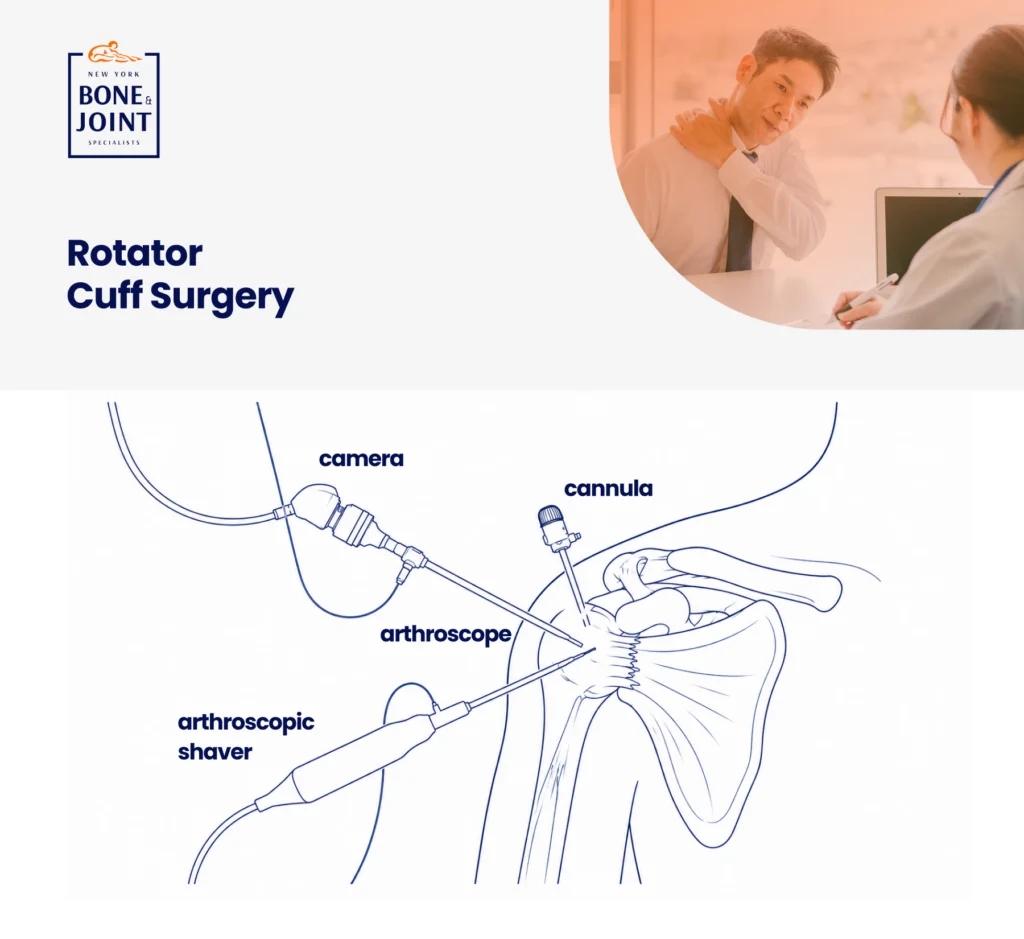
The Procedure: What Happens During Rotator Cuff Repair
Rotator cuff repair at New York Bone & Joint is performed entirely arthroscopically. Arthroscopy is a minimally invasive approach using two or three small portals, a camera, and specialized instruments. Patients go home the same day. Most procedures take between 60 and 120 minutes depending on tear size, number of tendons involved, and whether concurrent pathology is addressed. [2]
Your surgeon will:
- Create two or three small portals around the shoulder, typically less than a centimeter each.
- Perform a complete arthroscopic survey of the entire shoulder: The rotator cuff tendons, the labrum, the biceps anchor, the subacromial space, the articular surfaces, and the joint capsule. Concurrent pathology (biceps tendon involvement, partial SLAP tears, impingement) is identified and addressed in the same procedure.
- Prepare the tendon footprint: The footprint is the bony attachment site on the humeral head. That area is debrided to create a vascular bed that supports tendon healing. The quality and extent of footprint preparation is one of the primary determinants of healing rate.
- Mobilize the tendon: For larger and massive tears, the retracted tendon must be systematically freed from surrounding adhesions and scar tissue until it can be advanced to the footprint without tension. This mobilization step is the most technically demanding aspect of large tear repair, and the ability to achieve it arthroscopically requires significant surgical experience.
- Place suture anchors and repair the tendon: Suture anchors are placed in precise positions across the footprint. For most complete tears, New York Bone & Joint surgeons use a double-row or transosseous equivalent construct, placing a medial row of anchors at the articular margin and a lateral row at the footprint edge, to maximize footprint coverage and compression of the tendon against bone. [8] Single-row repair is used selectively where tissue or anatomy requires it.
- Close the portals and apply a surgical dressing. You leave with a sling and a clear protocol for starting physical therapy.
“A nuance that shapes every large tear repair: double-row technique creates superior footprint coverage. This optimizes healing, but only when the tendon has sufficient mobility to reach the lateral row without tension. A tendon under tension at the repair site is a repair that is at risk of pulling off. Sometimes the most important intraoperative decision is recognizing that a double-row construct is not achievable without compromising the repair and accepting a single-row construct that holds, rather than a double-row construct that fails. That judgment cannot be made from an MRI. It’s made in the operating room when the tendon is directly inspected and probed. Ultimately, though, the studies have not shown a clinically significant difference in functional outcomes between the two techniques, though double-row provides superior structural healing rates in larger tears. [14] Be that as it may, an experienced shoulder surgeon will know how to utilize both techniques for the benefit of the individual patient.” —Leon Popovitz, MD
Concurrent Procedures Frequently Performed with Rotator Cuff Repair
The shoulder arthroscopy performed during rotator cuff repair allows a complete inspection of the entire joint. Several conditions are commonly found and treated in the same operative session:
- Biceps tendon pathology: The long head of the biceps is a frequent source of anterior shoulder pain and is commonly involved in the same pathological process as rotator cuff tears. Biceps tenotomy (releasing the tendon) or biceps tenodesis (reattaching it lower on the arm) is performed based on patient age, activity level, and tissue condition. [10]. This should not be done routinely. The indications are very specific and requires the patient to be experiencing biceps pain with biceps damage. If that isn’t present then including biceps surgery would subject the patient to unnecessary additional surgery.
- Subacromial decompression: Bone spurs on the undersurface of the acromion are removed to create more space for the repaired tendon and reduce the impingement that contributed to the original tear.
- Partial SLAP or labral tears: Labral pathology is identified and addressed where clinically indicated. Typically a debridement of the labral tearing is performed, especially in older patients because studies have shown that when a SLAP repair is done at the same time as a full rotator cuff repair then the patient may experience stiffness post operatively. [13]
- Loose bodies and synovitis: Inflammatory tissue and loose fragments are removed as part of the complete joint survey.
All concurrent procedures are discussed with you before surgery. We do not add procedures during the case without having established the clinical basis for them.
Recovery and Rehabilitation: What to Expect
Rotator cuff repair requires a more structured recovery than most shoulder procedures. The repaired tendon must go through a biological healing process and lacks mechanical strength immediately after surgery. The rehabilitation protocol is designed to protect the repair during healing while preventing the stiffness and weakness that compromise the final result.
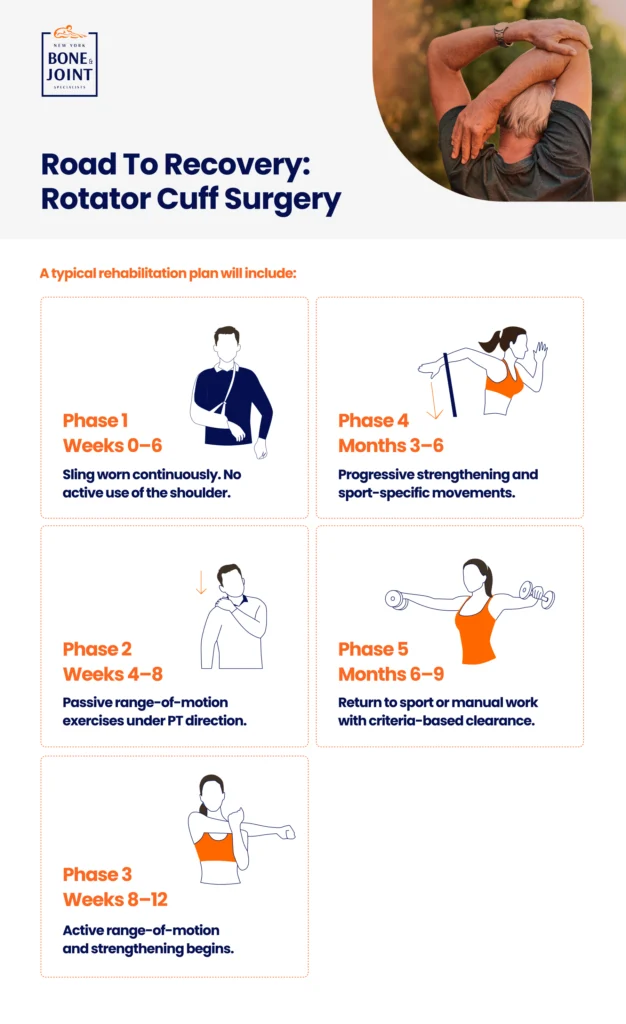
| Phase | Timeframe | Goals & Activities |
| Protection | Weeks 0–6 | Sling worn continuously. Pendulum exercises begin day 1–2 to prevent stiffness. No active use of the repaired shoulder. Ice and elevation for swelling control. Desk work typically by week 2–3. This phase is non-negotiable: removing the sling too early is the primary cause of early re-tear. |
| Passive Motion | Weeks 4–8 | Passive range-of-motion exercises under a physical therapist’s direction. The therapist moves your arm: you do not use your own muscle. Gradual progression of elevation and rotation. Sling weaned as directed by your surgeon. |
| Active Motion | Weeks 8–12 | Active range-of-motion begins. Therapist-guided strengthening of the periscapular muscles. Full elevation target by week 12 in most cases. |
| Strengthening | Months 3–6 | Progressive rotator cuff and deltoid strengthening. Resistance exercises begin. Sport-specific or work-specific movements introduced. Overhead activity with light loads. |
| Return to Activity | Months 6–9 | Return to sport, overhead athletics, or manual work with full strength. Criteria-based clearance: strength testing, range-of-motion documentation, and physician sign-off required. Not time-based alone. [12] |
| Why the sling protocol is the most important thing you will do after surgeryThe repaired tendon has no mechanical strength for the first six to eight weeks. During this period, the biology of healing (vascular ingrowth, cellular repair, early collagen formation) occurs at the repair site. Any significant load applied during this window doesn’t stress the tendon but rather the suture anchors and the sutured tissue, which are not designed to substitute for a healed tendon. Patients who remove their sling early, reach overhead, or use the arm actively during the protection phase are the ones who re-tear. The sling is not comfort equipment. It is surgical protection. |
In-House Physical Therapy: Why Coordinated Rehabilitation Determines the Outcome
After rotator cuff repair, the quality of rehabilitation is as important as the quality of the surgery. The two are inseparable in determining the final outcome. A technically perfect repair can fail if the post-operative protocol is wrong. And a well-protected repair can still produce a stiff, weak shoulder if rehabilitation is too aggressive too early or too passive too long.
At New York Bone & Joint, your physical therapist and your surgeon are in the same center. Before your first PT session, your therapist has already reviewed your operative report, confirmed the repair size and technique, and spoken with your surgeon about the specific protocol for your tear. The protection phase, the passive motion timeline, the strengthening progression, and the return-to-activity milestones are all calibrated to what was done in the operating room instead of to a generic template.
For patients returning to overhead sport or manual work, our team uses objective functional testing (such as strength symmetry indices, range-of-motion measurements, and sport-specific or work-specific movement assessments) to determine readiness. We do not clear patients based on how much time has passed. We clear them based on what their shoulder can actually do.
Why Choose New York Bone & Joint for Rotator Cuff Repair?
| NYBJ Advantage | What It Means for You |
| 2–4% re-tear rate (vs. published 10–20%) | Based on our own surgical outcome data. Achieved through precise footprint reconstruction, optimal suture anchor placement, tendon mobilization technique, and a coordinated post-operative rehabilitation protocol. |
| 94% patient satisfaction rate | Based on our own surgical outcome data: significant improvements in pain, strength, and range of motion. Not a satisfaction survey about the waiting room. A clinical outcome measure. |
| Full-spectrum tear capability | We repair the full range: partial-thickness, small, medium, large, and massive tears. Patients referred elsewhere for ‘irreparable’ tears are evaluated individually. We have repaired tears that other surgeons declined or failed to repair. |
| All-arthroscopic technique | No open surgery. Small portals, minimal tissue disruption, faster recovery, lower infection risk, and equivalent or better outcomes compared to open repair for the full spectrum of tears. |
| Double-row repair where indicated | Maximizes footprint coverage and compression of the tendon against bone, improving healing rate for medium and large tears. Single-row used selectively when anatomy or mobility requires it. [8] |
| Intraoperative tissue judgment | The repair decision is finalized in the operating room. Tissue quality, tendon mobility, and footprint coverage are assessed directly and not from MRI alone. This is the difference between a surgeon who repairs rotator cuffs and a specialist who understands them. |
| In-house PT — same center | Your surgeon and physical therapist communicate directly. Protocol is calibrated to your specific repair. The sling timeline, the progression milestones, and the return-to-activity clearance are all coordinated from day one. |
| Prompt consultations | Acute shoulder injuries seen quickly. Imaging coordinated immediately. For large tears where timing matters, we do not create delays. |
| The bottom lineA rotator cuff repair isn’t a commodity procedure. The re-tear rate gap (2–4% at New York Bone & Joint vs. 10–20% in the published literature) isn’t a marketing claim. It’s the documented result of surgical technique, patient selection, and rehabilitation coordination done consistently over 20 years. When you choose who repairs your rotator cuff, you are choosing that result. |
Risks & Considerations
Rotator cuff repair is a well-established and generally safe procedure. As with any surgery, there are risks that should be understood before proceeding. [11]
- Re-tear or incomplete healing: The most significant risk specific to rotator cuff repair. Published re-tear rates range from 10–20% overall, rising to 20–40% for massive tears in the general population. [4] [6] At New York Bone & Joint, based on our own surgical outcome data, our re-tear rate is 2–4% for non-massive tears. Risk of re-tear is higher for larger tears, patients over 65, and patients with significant fatty infiltration on MRI. Your surgeon will discuss your specific re-tear risk before the procedure.
- Stiffness (arthrofibrosis): Some patients develop excessive scar tissue post-operatively, particularly those who progress too slowly through the motion phase or who have a biological predisposition to fibrosis. Early supervised PT with a protocol specific to your repair type significantly reduces this risk. In rare cases, a manipulation under anesthesia may be necessary. This is very uncommon in our practice.
- Infection: Rare with arthroscopic procedures (less than 1% [11]). Strict sterile technique and post-operative care instructions minimize this risk.
- Nerve injury: Very rare with standard shoulder arthroscopy portals. Discussed in detail for complex large and massive tear reconstructions.
- Non-surgical alternative: For partial tears, degenerative tears with minimal functional limitation, and patients who are not surgical candidates, a structured physical therapy program for rotator cuff strengthening and scapular stabilization can effectively manage symptoms without surgery. [9] We will discuss this pathway honestly if it applies to your situation.
At your consultation, your surgeon will walk through the specific risks relevant to your tear size, your anatomy, and your individual health profile.
References
- American Academy of Orthopaedic Surgeons. Rotator Cuff Tears. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/rotator-cuff-tears
- American Academy of Orthopaedic Surgeons. Rotator Cuff Repair Surgery. OrthoInfo. orthoinfo.aaos.org/en/treatment/rotator-cuff-repair-surgery
- American Orthopaedic Society for Sports Medicine (AOSSM). Rotator cuff repair outcomes. aossm.org
- Kakoi H et al. Clinical outcomes of arthroscopic rotator cuff repair: a retrospective comparison of double-layer, double-row and suture bridge methods. BMC Musculoskelet Disord. 2018. pmc.ncbi.nlm.nih.gov/articles/PMC6134589
- Abrams GD et al. Arthroscopic repair of full-thickness rotator cuff tears. Am J Sports Med. 2014. pubmed.ncbi.nlm.nih.gov/24733157
- Galatz LM et al. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg. 2004. pubmed.ncbi.nlm.nih.gov/14960664
- Matthewson G et al. Partial-thickness rotator cuff tears: current concepts. Adv Orthop. 2015. pubmed.ncbi.nlm.nih.gov/26171251
- Boileau P et al. Arthroscopic repair of full-thickness tears of the supraspinatus: does the type of repair influence the outcome? Am J Sports Med. 2005. pubmed.ncbi.nlm.nih.gov/15930531
- American Academy of Orthopaedic Surgeons. Shoulder Impingement/Rotator Cuff Tendinitis. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/shoulder-impingement-rotator-cuff-tendinitis
- Sciascia AD et al. Indications for Biceps Tenodesis in Injured Overhead Throwing Athletes Lack Consensus: A Systematic Review and Cross-Sectional Survey. Arthrosc Sports Med Rehabil. 2025. pmc.ncbi.nlm.nih.gov/articles/PMC12276543
- Shin JJ et al. Complications After Arthroscopic Shoulder Surgery: A Review of the American Board of Orthopaedic Surgery Database. J Am Acad Orthop Surg Glob Res Rev. 2018. pmc.ncbi.nlm.nih.gov/articles/PMC6336573
- Elsenbeck MJ et al. Return to Sports After Shoulder Stabilization Surgery for Anterior Shoulder Instability. Curr Rev Musculoskelet Med. 2017. pmc.ncbi.nlm.nih.gov/articles/PMC5685962
- Abbot AE et al. Arthroscopic treatment of concomitant SLAP lesions and rotator cuff tears in patients over the age of 45 years. Am J Sports Med. 2009. pubmed.ncbi.nlm.nih.gov/19364887
- Millett PJ et al. Clinical and structural outcomes after arthroscopic single-row versus double-row rotator cuff repair: a systematic review and meta-analysis of level I randomized clinical trials. J Shoulder Elbow Surg. 2014. pubmed.ncbi.nlm.nih.gov/24411671
- Melis B et al. Natural History of Fatty Infiltration and Atrophy of the Supraspinatus Muscle in Rotator Cuff Tears. Clin Orthop Relat Res. 2010. pubmed.ncbi.nlm.nih.gov/20094853
- Gladstone JN et al. Fatty infiltration and atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with poor functional outcome. Am J Sports Med. 2007. pubmed.ncbi.nlm.nih.gov/17337727


