Shoulder Arthroscopy NYC — Minimally Invasive Shoulder Surgery at New York Bone & Joint
Written by: Dr. Popovitz.
Board-Certified Orthopedic Surgeon | Fellowship-Trained Sports Medicine, NYU Langone Medical Center | FAAOS
Co-Founder, NY Bone & Joint Specialists | Lenox Hill Hospital - Northwell Health
Recognized: New York Magazine Best Doctor | New York Times Super Doctor | IAOS Leading Physician of the World | IAOS Top Orthopedic Surgeon in New York
Date Published: May 5, 2026
Last Updated: June 26, 2026
Last Medically Reviewed: June 26, 2026
This page has been written and reviewed by a fellowship-trained, board-certified orthopedic surgeon with over 20 years of clinical experience. All clinical claims are supported by peer-reviewed literature and current AAOS and AOSSM guidelines. See References section below.
At a glance
- What it is: A minimally invasive surgical procedure using a small camera (arthroscope) and small portals to treat injuries inside the shoulder joint, without open surgery.
- What it treats: Rotator cuff tears, SLAP tears, labral tears, shoulder instability (Bankart lesions), biceps tendon pathology, impingement, and loose bodies.
- Who performs it: Dr. Leon Popovitz, MD and the New York Bone & Joint fellowship-trained surgical team: board-certified orthopedic surgeons with subspecialty training in shoulder surgery. 20+ years of shoulder arthroscopy experience. Surgery at Lenox Hill Hospital.
- Where: Consultations, imaging, and physical therapy at two Manhattan offices: Upper East Side (1198 Third Ave) and Midtown (425 Madison Ave). Surgery performed at Lenox Hill Hospital.
- Recovery: Sling: 1–2 weeks for impingement/AC joint procedures; 4–6 weeks for rotator cuff repair and SLAP repair. Return to desk work: typically within 1–2 weeks. Return to overhead sport: 4–6 months for impingement; 6+ months for rotator cuff repair; 6–9 months for SLAP repair. All clearance is criteria-based, not time-based alone.
- Typical candidates: Patients with confirmed structural shoulder pathology on MRI who have not responded to physical therapy and/or injections, or who have sustained acute traumatic injuries requiring surgical repair.
- Insurance: Most major insurance accepted. Coverage verified before your procedure.
- NYBJ outcomes: Based on our own surgical outcome data (rotator cuff re-tear rate 2–4%; meniscus repair healing rate 95%; return to competitive throwing after SLAP repair 90%) compared to published benchmarks of 10–20% re-tear, 70–90% meniscus healing, and 75–85% return-to-throwing rates.
Book a consultation
Prompt Appointments Available
Upper East Side: 1198 Third Ave | Midtown: 425 Madison Ave
Surgery performed at Lenox Hill Hospital - Northwell Health
About this page
About This Page: This page was written and is maintained by Leon Popovitz, MD, a board-certified orthopedic surgeon and co-founder of New York Bone & Joint Specialists, a private orthopedic surgery and sports medicine practice with two locations on the Upper East Side and in Midtown. Dr. Popovitz was trained in sports medicine at NYU Langone Medical Center and has specialized in shoulder and knee surgery for over 20 years. Shoulder arthroscopy (including rotator cuff repair, SLAP repair, Bankart repair, and biceps tenodesis) is performed by Dr. Popovitz at Lenox Hill Hospital, part of the Northwell Health system. New York Bone & Joint Specialists is independent of hospital systems and operates as a private practice serving patients across New York City and the surrounding region. Dr. Popovitz has served as a team physician for professional sports events including the US Open Tennis Championships and has treated athletes at recreational, collegiate, and professional levels throughout his career.
If you have already been evaluated and recommended for shoulder arthroscopy, choosing the right surgical team is the most important decision you will make.
New York Bone & Joint Specialists is a team of orthopedic surgeons and sports medicine physicians built around our founder’s, Dr. Leon Popovitz, MD, core belief: that preserving your body’s tissues is the foundation of long-term health and performance. From your first consultation through your last physical therapy session, every provider at New York Bone & Joint is committed to protecting your cartilage, ligaments, tendons, and muscle because healthy tissue is what keeps you active for life. When surgery is the right answer, it’s because it’s the most effective way to preserve that tissue, restore function, and protect the joint for the long term.
Dr. Popovitz is a board-certified orthopedic surgeon fellowship-trained in sports medicine at NYU Langone Medical Center and a Fellow of the American Academy of Orthopaedic Surgeons (FAAOS). Shoulder surgery is one of his primary subspecialties. Over more than 20 years in practice, he has personally treated Olympic and professional athletes and active New Yorkers across all levels of sport who simply need to get back to the life they love. His clinical approach brings firsthand surgical insight into the specific challenges that determine shoulder outcomes: from the decision between SLAP repair and biceps tenodesis, to identifying concurrent instability during arthroscopy, to the tissue quality assessment that distinguishes a rotator cuff worth repairing from one requiring a different approach.
Dr. Popovitz has been recognized by New York Magazine as a Best Doctor, by the New York Times as a Super Doctor, and by the International Association of Orthopedic Surgeons as both a Leading Physician of the World and Top Orthopedic Surgeon in New York. Every physician he has brought to New York Bone & Joint practices with that same depth of clinical judgment.
Already evaluated and recommended for arthroscopic shoulder surgery? You don’t need to start over. New York Bone & Joint offers prompt surgical consultations and second opinions so you can move forward with confidence, or get the clarity you need before making a decision.
Dealing with a shoulder injury and not yet sure what you need? Our sports medicine physicians can evaluate you same day or next day if needed. If a surgical consultation is warranted, one of our orthopedic surgeons will see you promptly. You are already with the team best equipped to take the next step.
Introduction
If you’ve been told you need shoulder arthroscopy or you’re researching your options after a shoulder injury, the most important thing to know is this: arthroscopic shoulder surgery is one of the most technically advanced and least invasive procedures in orthopedics, and outcomes are far better than most patients expect when performed by a specialist with genuine subspecialty depth in the shoulder. At New York Bone & Joint Specialists, our fellowship-trained shoulder surgeons have performed arthroscopic procedures for over 20 years, treating rotator cuff tears, SLAP tears, labral injuries, shoulder instability, and persistent shoulder pain that hasn’t responded to conservative treatment. [1]
New York Bone & Joint surgeons perform shoulder arthroscopy at Lenox Hill Hospital, while consultations, imaging, and physical therapy take place at our Upper East Side and Midtown offices. This model gives patients the best of both worlds: the personal attention and accessibility of a dedicated private practice, combined with the surgical infrastructure of a top-tier Manhattan hospital.
Prompt access to expert orthopedic care is a cornerstone of how New York Bone & Joint operates. If you’ve already been evaluated elsewhere and recommended for shoulder arthroscopy, you don’t need to wait weeks to see a surgeon. New York Bone & Joint offers prompt surgical consultations and second opinions so you can move forward with confidence or get the clarity you need before making a decision.
If you have sustained an acute shoulder injury and are not yet sure what you are dealing with, one of our sports medicine physicians can evaluate you quickly. If that evaluation indicates a surgical consultation is warranted, an appointment with one of our orthopedic surgeons is arranged promptly.
What Is Shoulder Arthroscopy?
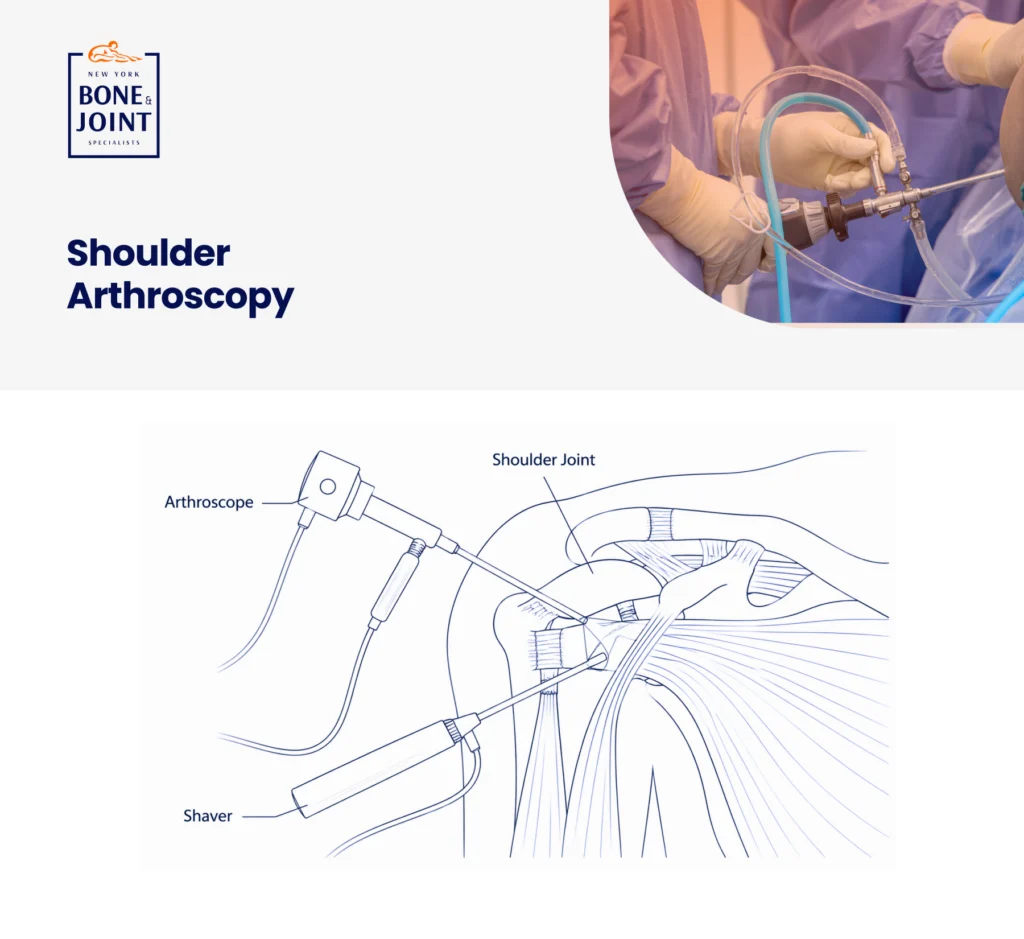
Shoulder arthroscopy is a minimally invasive surgical technique that allows the surgeon to see inside your shoulder joint and treat a wide range of problems. Two or three small incisions (cuts that are each approximately the size of a buttonhole) are created around the shoulder. A tiny camera called an arthroscope is inserted through one cut, projecting a real-time image of the joint interior onto a monitor. Surgical instruments are passed through the other cuts to perform the procedure. [1]
Because the incisions are small, tissue disruption is minimal. Patients go home the same day. Swelling resolves faster, rehabilitation begins sooner, and return to activity is significantly quicker than with open shoulder surgery.
The shoulder is an exceptionally complex joint, offering more range of motion than any other joint in the body, which also makes it uniquely vulnerable to injury. The arthroscope allows a trained shoulder surgeon to inspect and treat structures that cannot be reliably assessed any other way: the full extent of the rotator cuff, the labrum, the biceps anchor, the joint capsule, and the articular surfaces all within the same procedure.
Conditions Treated With Shoulder Arthroscopy
Shoulder arthroscopy is not a single procedure. It’s a surgical approach used to treat several distinct conditions of the shoulder joint and surrounding structures. The most common include:
Rotator Cuff Tears. The rotator cuff is a group of four muscles and tendons that stabilize the shoulder and enable overhead and rotational movement. When one or more tendons tear, either from acute injury or gradual degeneration, arthroscopic repair reattaches the tendon to the bone using suture anchors, restoring strength and eliminating pain. [3] New York Bone & Joint surgeons perform all-arthroscopic repairs for the full spectrum of rotator cuff tears, from small partial-thickness tears to large full-thickness tears, adapting technique to what the tissue and findings require.
“A decision that frequently cannot be made from MRI alone is whether a partial-thickness rotator cuff tear needs to be debrided or repaired. An MRI may show a 50% thickness tear, but the quality of the tissue and actual boney coverage need to be assessed intraoperatively. We always go in with the goal of preserving your tissue and prepared to perform whatever level of repair the findings require.” — Leon Popovitz, MD
SLAP Tears. The labrum is the cartilage ring that deepens the shoulder socket and anchors the biceps tendon. A SLAP (superior labrum anterior to posterior) tear is a tear of the top of the labrum where the biceps tendon attaches to the glenoid. SLAP tears commonly affect overhead athletes, throwing athletes, and patients who sustain a fall on an outstretched arm. [2]
Arthroscopic SLAP repair reattaches the labrum using suture anchors, restoring the biceps anchor and eliminating the pain, clicking, and weakness that characterize this injury. For overhead athletes, SLAP repair supports return to competitive throwing at 6–9 months in appropriately selected patients. [7] Based on New York Bone & Joint’s own surgical outcome data, 90% of our overhead athlete patients return to competitive throwing after SLAP repair, compared to published return-to-sport rates of 75–85% in the literature.
“An important clinical nuance with SLAP tears: not every labral finding on MRI is a true symptomatic SLAP tear, and not every symptomatic SLAP tear should be repaired in the same way. In patients over 35 or with significant biceps tendon involvement, a biceps tenodesis often provides equally good or better pain relief with a more predictable healing response. The decision is an intraoperative one: we assess the tissue quality, the integrity of the biceps anchor, and the characteristics of the tear directly. An MRI can raise the suspicion, but the operating room is where the definitive assessment happens.” — Leon Popovitz, MD
Shoulder Instability: Bankart Lesions & Labral Tears. When the shoulder dislocates, it commonly tears the anterior and inferior labrum, creating what’s called a Bankart lesion. Without repair, the recurrence rate in patients under 25 exceeds 70%. [8] Arthroscopic Bankart repair reattaches the torn labrum and tightens the stretched capsule, restoring the shoulder’s natural restraint mechanism.
For patients with significant glenoid bone loss, additional procedures may be required, which our surgeons will assess and discuss before surgery.
“An important nuance: often during an arthroscopic Bankart repair and stabilization procedure, we find the tear extends superiorly and undermines the biceps tendon attachment, creating a SLAP tear as well. We always perform a complete arthroscopic survey of the entire joint and are prepared to repair whatever we find.” — Leon Popovitz, MD
Biceps Tendon Pathology. The long head of the biceps tendon originates at the top of the shoulder and is a frequent source of anterior shoulder pain, particularly in patients with rotator cuff pathology or SLAP tears. Arthroscopy allows direct assessment and treatment, including biceps tenotomy (releasing the tendon) or biceps tenodesis (reattaching it lower on the arm). [10] The choice depends on patient age, activity level, and the condition of the remaining tissue.
Shoulder Impingement & Bursitis. When bone spurs develop over the rotator cuff and the bursa becomes inflamed and thickened, it can cause persistent pain and limited motion. Arthroscopic subacromial decompression removes the inflamed bursa and creates more space for the rotator cuff tendons, relieving impingement.
AC Joint Arthroplasty (Mumford Procedure). Erosion of the AC joint from lifting weights or overhead activities (AC joint osteolysis) or arthritis of the acromioclavicular (AC) joint can cause chronic pain with overhead activity. Arthroscopic AC joint arthroplasty removes a small portion of the end of the clavicle (collarbone), eliminating the bony contact that causes pain.
Loose Body Removal. Fragments of bone or cartilage floating within the shoulder joint causing catching, locking, or sudden sharp pain can be identified and removed arthroscopically.
Are You a Candidate for Shoulder Arthroscopy?
Not every shoulder problem requires surgery, and at New York Bone & Joint, we will never recommend arthroscopy unless it is genuinely the right answer for your specific situation. Arthroscopy is typically recommended when:
- You have a confirmed full-thickness or significant partial-thickness rotator cuff tear that has not improved with physical therapy and injections [3]
- You have a confirmed SLAP tear with mechanical symptoms (pain with overhead activity, clicking, weakness) that has not responded to conservative management [2]
- You have recurrent shoulder dislocations, confirmed labral tearing on MRI, and are an active patient for whom continued non-operative management is inadequate [4] [8]
- You have persistent shoulder impingement or bursitis that has failed a course of physical therapy and cortisone injection
- You have confirmed biceps tendon pathology causing anterior shoulder pain and functional limitation [10]
- Imaging has identified a structural problem that cannot be adequately treated non-surgically
Shoulder arthroscopy is generally not recommended for patients with pain alone and no confirmed structural diagnosis, patients who have not completed an appropriate course of conservative treatment, or patients with significant glenohumeral arthritis where joint preservation is no longer realistic. At your consultation, we’ll review your imaging, your symptom history, and your activity goals. Then, we’ll give you a straight answer about whether surgery is the right next step.
All the while, New York Bone & Joint surgeons’ core focus will always be to preserve your own tissue. We believe that is the key to the longevity of your joints and overall health.
| From Dr. Popovitz: Why the Right Diagnosis Changes Everything A 26-year-old tennis player came to see me after three to six months of shoulder pain that had been managed elsewhere as rotator cuff tendinitis. He had undergone a course of physical therapy and 2 cortisone injections, neither of which gave him any lasting relief. On examination, he had signs of a SLAP tear. We obtained an MRI for him which confirmed a Type II SLAP tear with a paralabral cyst (caused by the synovial fluid flowing through the tear). The cortisone injections were not indicated for this patient and not particularly appropriate for a young 26 year old. We performed an arthroscopic SLAP repair and decompressed his paralabral cyst. He returned to competitive tennis at eight months post-surgery. What stays with me from that case isn’t the surgery, it’s the wrong treatment he received and the delay in the repair (that might have been the cause of his cyst). Getting the right answer first and determining the appropriate treatment are what allows us to get people back to the life they want. — Leon Popovitz, MD |
The Procedure: What Happens During Shoulder Arthroscopy
Shoulder arthroscopy is typically performed under general anesthesia. In many cases, a regional nerve block (interscalene block) is used alongside general anesthesia to minimize medication required and significantly reduce post-operative pain. Most cases take between 30 minutes and 90 minutes.
Your surgeon will:
- Position the shoulder to optimize visualization and access to all structures
- Make two or three small incisions, typically less than a centimeter each, around the shoulder to optimize access to the specific structures being treated
- Insert the arthroscope to visualize the joint: the rotator cuff tendons, the labrum, the biceps anchor, the articular surfaces, the subacromial space, and the joint capsule
- Introduce surgical instruments through the incisions to perform the specific procedure, whether that’s a rotator cuff repair, SLAP repair, Bankart repair, biceps tenodesis, subacromial decompression, or other indicated procedure
- Use sterile saline solution continuously throughout the procedure to distend the joint for access and visibility
- Close the incisions with small absorbable sutures and apply a surgical dressing
You will be discharged home the same day in most cases. You will leave with a surgical dressing, a sling, and a clear plan for starting physical therapy.
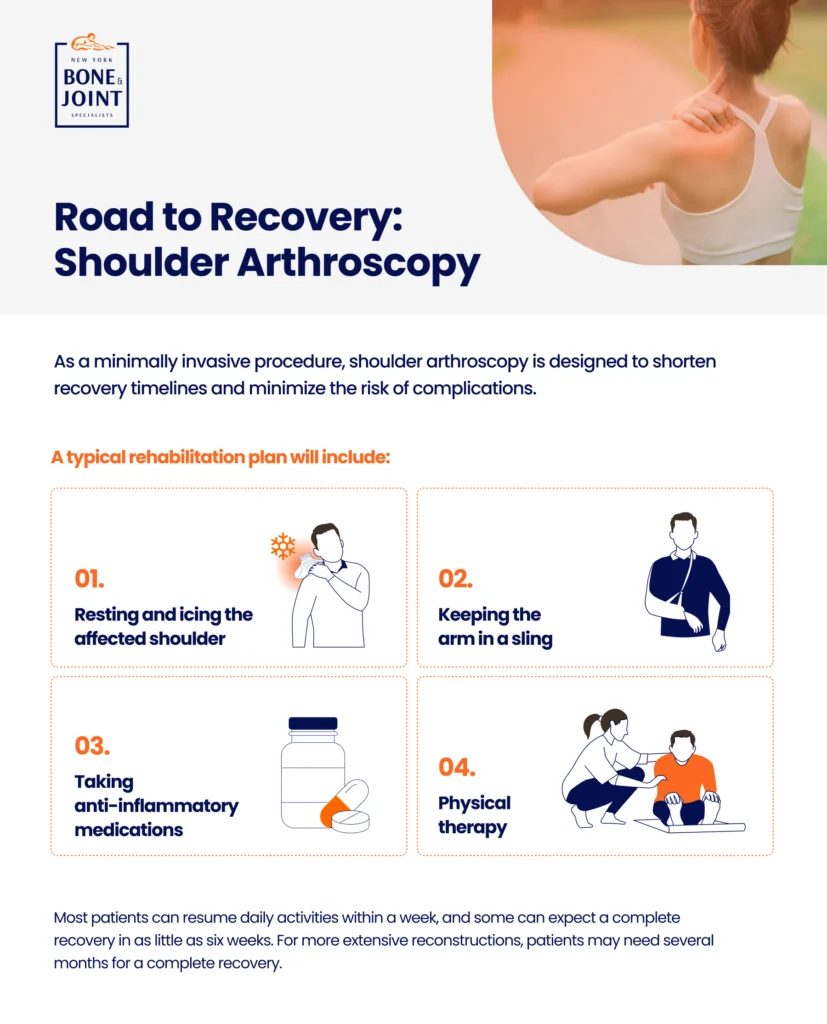
Recovery & Rehabilitation: What to Expect
Recovery timelines vary significantly depending on which procedure was performed. Below is a general guide. Your surgeon will provide a procedure-specific protocol at your pre-operative appointment.
| Timeframe | What to Expect |
| Weeks 1–2 | Sling immobilization if indicated. Ice and rest for pain and swelling management. Pendulum exercises begin day 1–2 to prevent stiffness. Return to desk work typically by week 2 for less involved procedures. |
| Weeks 3–6 | Progressive passive range-of-motion under PT direction. Sling weaning begins. Timeline varies by procedure (rotator cuff repairs require longer immobilization than SLAP repairs). Strengthening not yet started. |
| Weeks 6–12 | Active range-of-motion restored. Progressive strengthening begins. Stationary bike and walking for cardiovascular maintenance. |
| Months 3–4 | Sport-specific strengthening for throwing and overhead athletes. Rotational strengthening and scapular stabilization are priorities. |
| Months 4–6 | Return to light overhead activity and non-contact sport for less involved procedures (impingement, AC joint). Rotator cuff repairs require continued protection. |
| Months 6–9+ | Return to throwing, overhead sport, and full athletic activity for most procedures. Criteria-based clearance such as strength, range-of-motion testing, and physician sign-off rather than time alone. SLAP repairs in throwing athletes typically require 6–9 months before return to competitive throwing. [12] |
Patients who undergo subacromial decompression or AC joint resection typically return to desk work within one to two weeks and overhead activity within three to four months. Rotator cuff repair and SLAP repair require a more structured rehabilitation program and longer protected recovery. [5]
In-House Physical Therapy: Coordinated Rehabilitation at New York Bone & Joint
Your recovery after shoulder arthroscopy is as important as the surgery itself, and in shoulder surgery in particular, the rehabilitation protocol is one of the primary determinants of outcome. At New York Bone & Joint, your physical therapist and your surgeon are in the same center, and they communicate directly about your case from day one.
Before your first PT appointment, your New York Bone & Joint therapist has already reviewed your operative report and spoken with your surgeon. Your rehabilitation program is built around exactly what was done during your procedure, your surgeon’s protocol, and your specific recovery goals rather than a generic post-surgical template. When questions arise during your recovery, answers come the same day.
For throwing athletes and overhead sport athletes, our team uses sport-specific return-to-activity protocols with objective functional testing. The decision to return to your sport is based on what your shoulder can actually do, not just how much time has passed. [12]
Why Choose New York Bone & Joint Over a Hospital System?
If you’re considering arthroscopic shoulder surgery in New York City, you will likely compare us to major hospital systems like NYU Langone, Hospital for Special Surgery, or Mount Sinai. Here is what the comparison actually looks like:
| New York Bone & Joint Specialists | Major Hospital Systems | |
| Initial consultation wait | Prompt surgical consultations without the weeks-long waits of major hospital systems | Typically 4–8 weeks for an orthopedic consultation |
| Surgical facility | Lenox Hill Hospital, a premier Manhattan surgical facility | Varies by system and campus |
| Your evaluating physician | Is your surgeon, meaning you work with the same person, start to finish | May not be the surgeon who operates on you |
| PT after surgery | In-house, same center, same team; surgeon and therapist communicate directly | Often at a separate location, with separate providers |
| Imaging | Prompt MRIs at affiliated centers, coordinated by New York Bone & Joint | Often long waits; less personal coordination |
| Attention to your case | Private practice: your surgeon knows your case, history, and goals | High patient volume; potential secondary providers |
| Appointment accessibility | Direct access to your care team with questions | Communication through referral and scheduling systems |
| The bottom line When surgery is the right answer, who does it for you is what matters most. New York Bone & Joint orthopedic surgeons’ core focus is on preserving your joint health for a long lifetime to come. You’ll see the same fellowship-trained orthopedic surgeon from your first consultation through your last PT session, with your PT team in the same center. Surgery is performed at Lenox Hill Hospital. Your surgeon and your physical therapist communicate directly and regularly. And when you need to be seen, you are not waiting weeks for an appointment. This is how orthopedic care should work. |
Risks & Considerations
Shoulder arthroscopy is one of the safest procedures in orthopedic surgery, with a very low overall complication rate. As with any surgical procedure, there are risks that should be understood before proceeding:
- Infection. Rare with arthroscopic procedures (less than 1% [9]). Strict sterile technique and post-operative care instructions minimize this.
- Nerve injury. The shoulder has several nerves in close proximity to surgical portals. The risk is very low in standard shoulder arthroscopy performed by an experienced surgeon, and is discussed in detail for complex reconstructive cases.
- Stiffness (arthrofibrosis). Some patients develop excessive scar tissue post-operatively, particularly after rotator cuff repair with prolonged immobilization. Early supervised PT significantly reduces this risk.
- Re-tear or incomplete healing. Rotator cuff repairs have a known re-tear rate that depends on tear size, tissue quality, patient age, and biology. [5] SLAP repairs in throwing athletes over 35 sometimes have lower success rates, depending upon the tear, which is why biceps tenodesis is sometimes preferred in that population. [11]
- Blood clots (DVT). Uncommon after shoulder surgery. Your surgeon will advise on activity and anticoagulation if relevant to your profile.
At your consultation, your surgeon will walk through the specific risks relevant to your procedure and your individual health profile.
References
- American Academy of Orthopaedic Surgeons. Shoulder Arthroscopy. OrthoInfo. orthoinfo.aaos.org/en/treatment/shoulder-arthroscopy
- American Academy of Orthopaedic Surgeons. SLAP Tears. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/slap-tears
- American Academy of Orthopaedic Surgeons. Rotator Cuff Tears. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/rotator-cuff-tears
- American Academy of Orthopaedic Surgeons. Shoulder Dislocation. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/dislocated-shoulder
- American Orthopaedic Society for Sports Medicine (AOSSM). Rotator cuff repair outcomes. aossm.org
- Francisco B et al. Clinical Outcomes of Arthroscopic Revision Rotator Cuff Repair. Indian J Orthop. 2023. pmc.ncbi.nlm.nih.gov/articles/PMC9941391
- Aarabi T et al. Return to Sport After Arthroscopic Superior Labral Anterior-Posterior Repair: A Systematic Review. Sports Health. 2019. pubmed.ncbi.nlm.nih.gov/31584340
- Steven LB et al. Incidence of Posterior Shoulder Instability in the United States Military: Demographic Considerations From a High-Risk Population. Am J Sports Med. 2021. pubmed.ncbi.nlm.nih.gov/33264052
- Jason JS et al. Complications After Arthroscopic Shoulder Surgery: A Review of the American Board of Orthopaedic Surgery Database. J Am Acad Orthop Surg Glob Res Rev. 2018. pubmed.ncbi.nlm.nih.gov/30680371
- American Academy of Orthopaedic Surgeons. Biceps Tendon Tear at the Shoulder. OrthoInfo. orthoinfo.aaos.org/en/diseases–conditions/biceps-tendon-tear-at-the-shoulder
- Justin WG et al. Management of Proximal Biceps Pathology in Overhead Athletes: What Is the Role of Biceps Tenodesis?. Am J Orthop (Belle Mead NJ). 2017. pubmed.ncbi.nlm.nih.gov/28235123
- Michael JE et al. Return to Sports After Shoulder Stabilization Surgery for Anterior Shoulder Instability. Curr Rev Musculoskelet Med. 2017. pubmed.ncbi.nlm.nih.gov/29076041
FAQs
Most shoulder arthroscopy procedures take between 30 and 90 minutes, depending on what needs to be addressed. A subacromial decompression for impingement is typically 30–45 minutes. Rotator cuff repair and SLAP repair take approximately 60–90 minutes. You will be in and out of the surgical facility the same day in most cases. [1]
Everyone leaves with a sling. How long you need it depends on your specific procedure. Patients who undergo subacromial decompression or AC joint resection may use a sling only for comfort and typically transition out of it within one to two weeks. Patients who have rotator cuff repair or SLAP repair are placed in a sling for approximately four weeks to protect the repair during early healing. Your surgeon will give you specific instructions before your procedure.
Patients with desk jobs typically return to work within one to two weeks after less involved procedures, and two to four weeks after rotator cuff or SLAP repair. Patients with physically demanding jobs requiring overhead lifting or manual labor may need three to six months depending on the procedure. Your surgeon will provide a return-to-work estimate specific to your procedure and job requirements.
After SLAP repair, most overhead athletes return to competitive throwing at six to nine months post-surgery, and based on New York Bone & Joint’s own outcome data, 90% of our overhead athlete patients achieve return to competitive throwing. [12] After rotator cuff repair, return to overhead sport depends on tear size and repair technique, but is typically six months or longer. Your surgeon will provide a realistic, individualized timeline before your procedure.
SLAP repair reattaches the torn labrum to the glenoid socket using suture anchors, restoring original anatomy; biceps tenodesis releases the biceps tendon from the shoulder and reattaches it lower on the arm, eliminating the pain at the damaged anchor point. In younger, high-demand overhead athletes, SLAP repair is generally preferred. In patients over 35 or those with significant biceps involvement, tenodesis typically provides equally good or better pain relief with a more reliable healing response. [11] The decision is made based on your anatomy, activity demands, and intraoperative findings.
For rotator cuff repair, studies in the literature report 85–90% satisfactory outcomes in appropriately selected patients [6], and based on New York Bone & Joint’s own surgical outcome data, our rotator cuff re-tear rate is 2–4%, compared to published benchmarks of 10–20%. Bankart repair for shoulder instability reduces re-dislocation risk to under 10% in appropriately selected patients. [4] For SLAP repair in overhead athletes, 90% of New York Bone & Joint patients return to competitive throwing based on our own case data compared to published rates of 75–85%. [7] SLAP repair outcomes vary more by patient age and sport demands; patients over 35 may achieve better outcomes with biceps tenodesis. Your surgeon will discuss realistic expectations for your specific case.
In most cases yes, and for labral conditions specifically, a high-field MRI or MRI arthrogram is often needed to reliably assess the labrum, since standard and low-field open MRI can miss subtle SLAP tears. New York Bone & Joint is affiliated with MRI facilities across NYC and can coordinate a prompt appointment in a location convenient to you. You don’t need to navigate the hospital system for your imaging.
Arthroscopic procedures for structural shoulder problems such as rotator cuff tears, SLAP tears, labral injuries, and instability are typically covered by major insurance plans when medically indicated. Our team will verify your coverage before your procedure and provide a clear picture of your out-of-pocket responsibility, if any, in advance.
Medically Reviewed by Dr. Popovitz.
You can book your appointment with New York Bone & Joint online by submitting the appointment request form here:
Book an appointmentOur Locations
-

Upper East Side: Full Service Orthopedic Center & Walk-In
1198 3rd Avenue, Between 69th and 70th Street New York, NY 10021Physician appointments: Mon–Fri 9am–5:30pm, Sat 8:30am–4:30pm
Physical therapy: Mon–Fri 7am–7pm, Sat 8am–2pmPhone: (212) 759-4553 -

Orthopedic Doctor Midtown Manhattan NYC — New York Bone & Joint Specialists
425 Madison Ave, Suite 200 (second floor) New York, NY 10017 (corner of East 49th Street)Physician appointments: Mon–Fri 8:00 am–6:00 pm
Physical therapy: Mon–Fri 7 am–7 pm, Sat 8 am–2 pmPhone: (212) 759-4553 -

Orthopedic Doctor Upper East Side NYC — New York Bone & Joint Specialists
130 E 67th St New York, NY 10065Physician appointments: Mon–Fri 8:00am–6pm, Sat 8:30am–4:30pm
Physical therapy: Mon–Fri 7am–7pm, Sat 8am–2pmPhone: (212) 759-4553